Biology 2404 A&P Basics Lab Exercise 17 Respiratory Dr. Weis
| Objectives | Background | Medical Terms | Activities | Applications | Careers | WWW | Review Questions |
Students should be able to:
* define respiration
* name, identify, and give the functions of the organs of the respiratory system
* Name and describe the four phases of respiration
* Name the peripheral and central controls of respiration
* Name two respiratory tests and their use
* Describe the structure and function of the respiratory membrane
Read related material in textbook
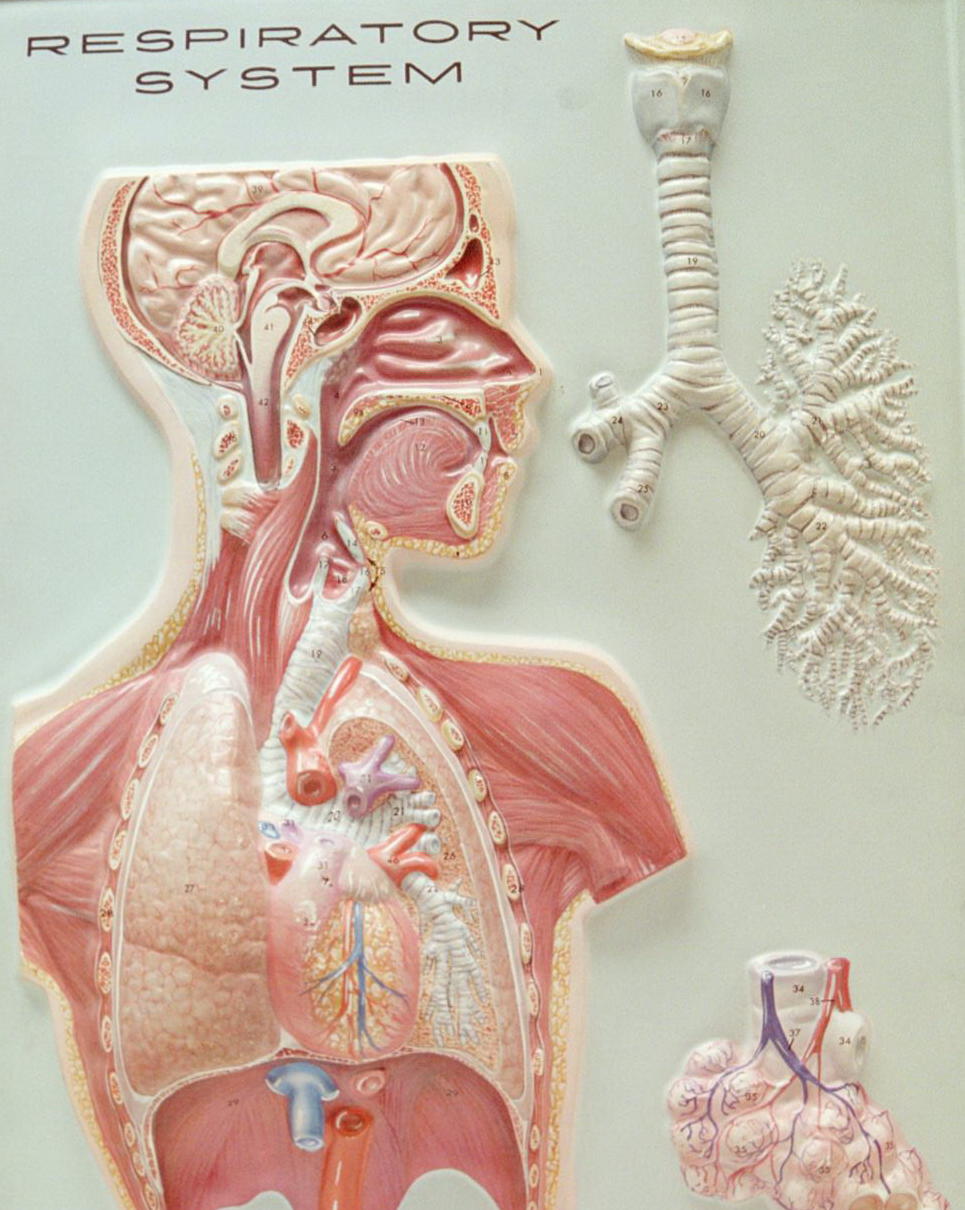
The respiratory system consists of conduction air passageways and gas exchange surfaces. Besides bringing air in for gas exchange of O2 and CO2, the respiratory system functions in olfaction, vocalization, immunity, and filters, warms, & moistens the air.
Anatomical means of dividing the system include the upper and lower respiratory tract and reflects the physical orientation as to structures that are located either outside or inside the chest cavity.
Upper respiratory structures are the nasal cavity, pharynx, larynx, and upper trachea. Lower respiratory tract structures are the lower trachea, bronchial tree, bronchioles, alveolar ducts, and aveoli.
The functional structures of the conduction passage ways are the: nasal cavity, pharynx, larynx, trachea, bronchial tree, bronchioles, and alveolar ducts.
The gas exchange surfaces are the alveoli of the lungs.
Respiration is the processes of exchanging respiratory gases, CO2 and O2.
The four phases of respiration are:
1) Pulmonary ventilation Bringing air in and out of the respiratory tract
2) External respiration Gas exchange between the alveoli and the blood
3) Internal respiration Gas transport in the blood
4) Cellular Respiration Gases used and created in metabolic reactions
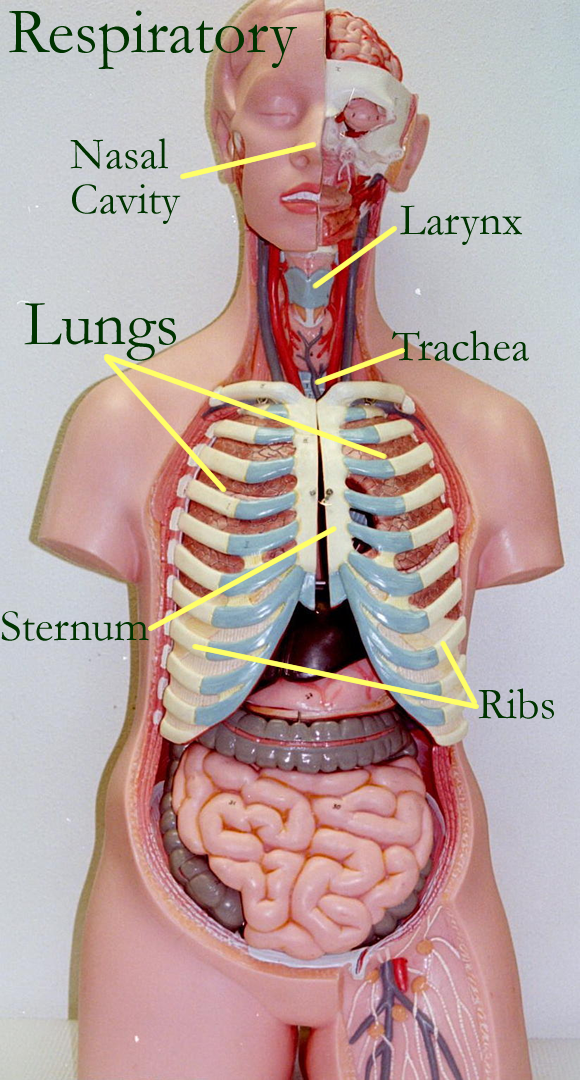
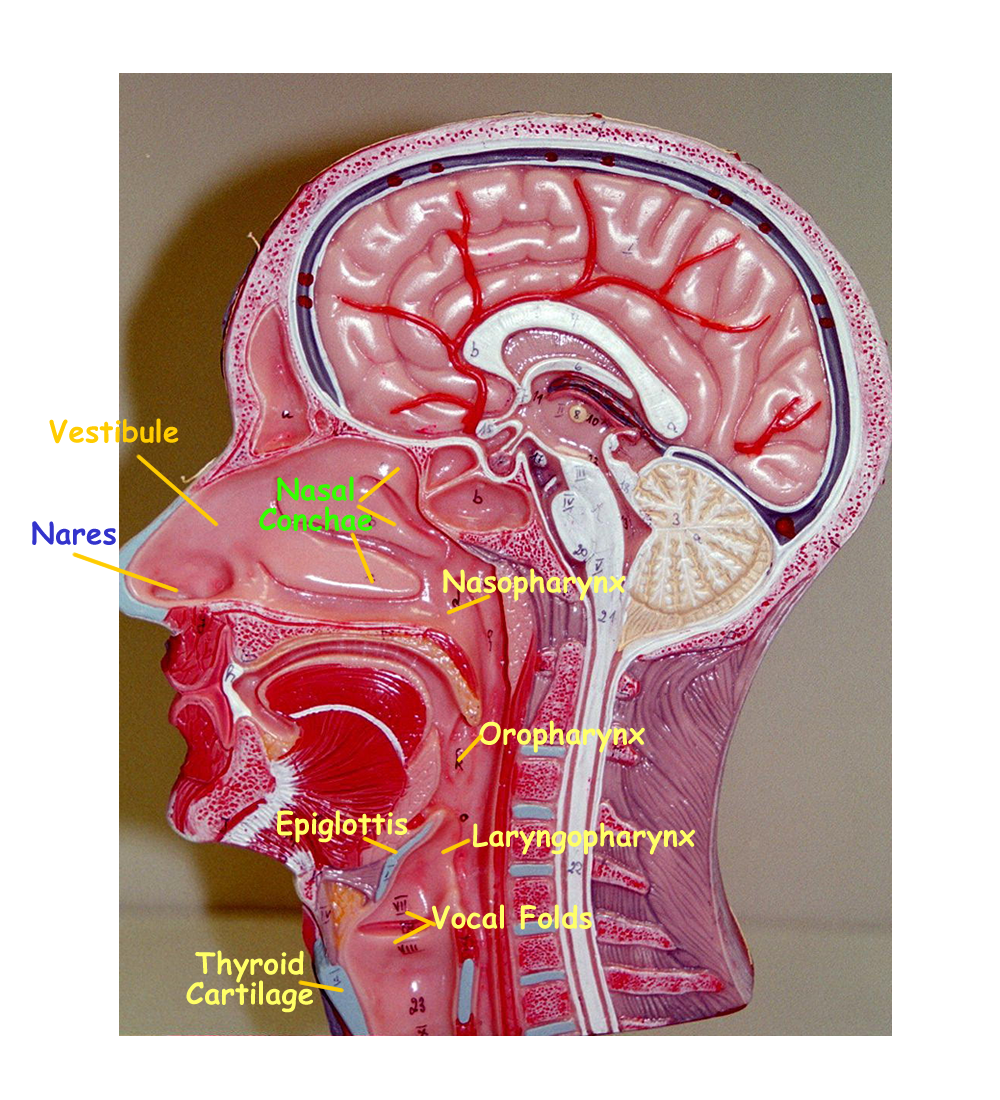
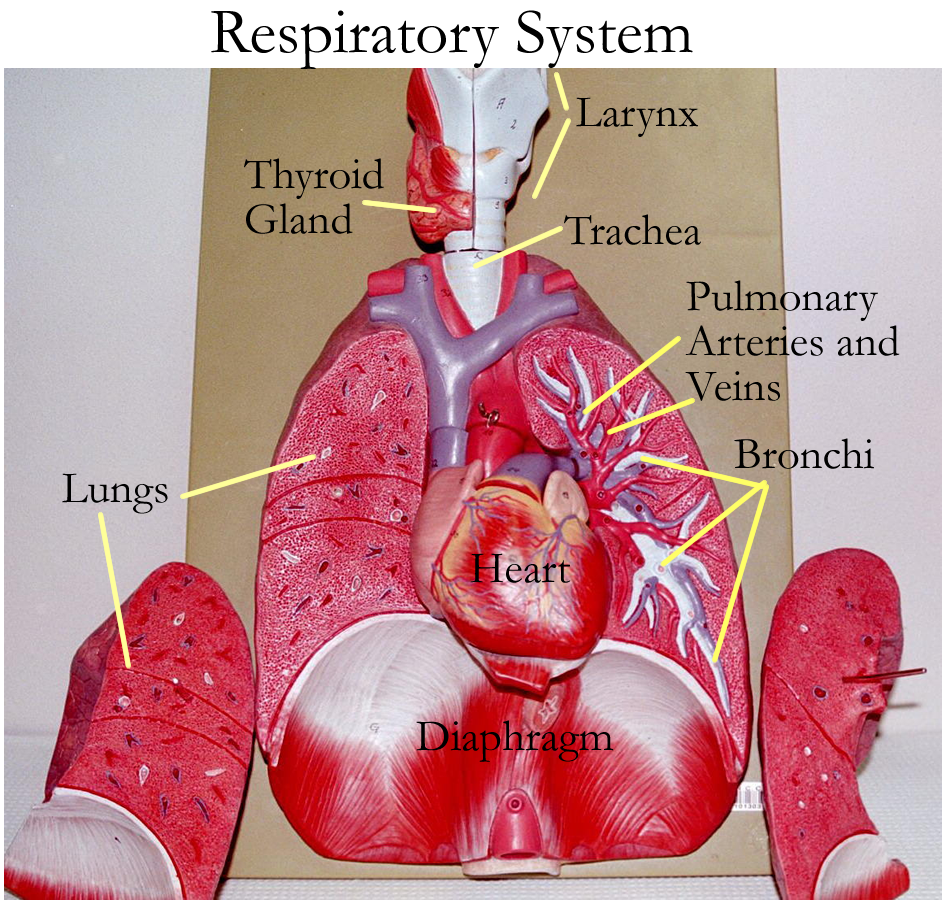
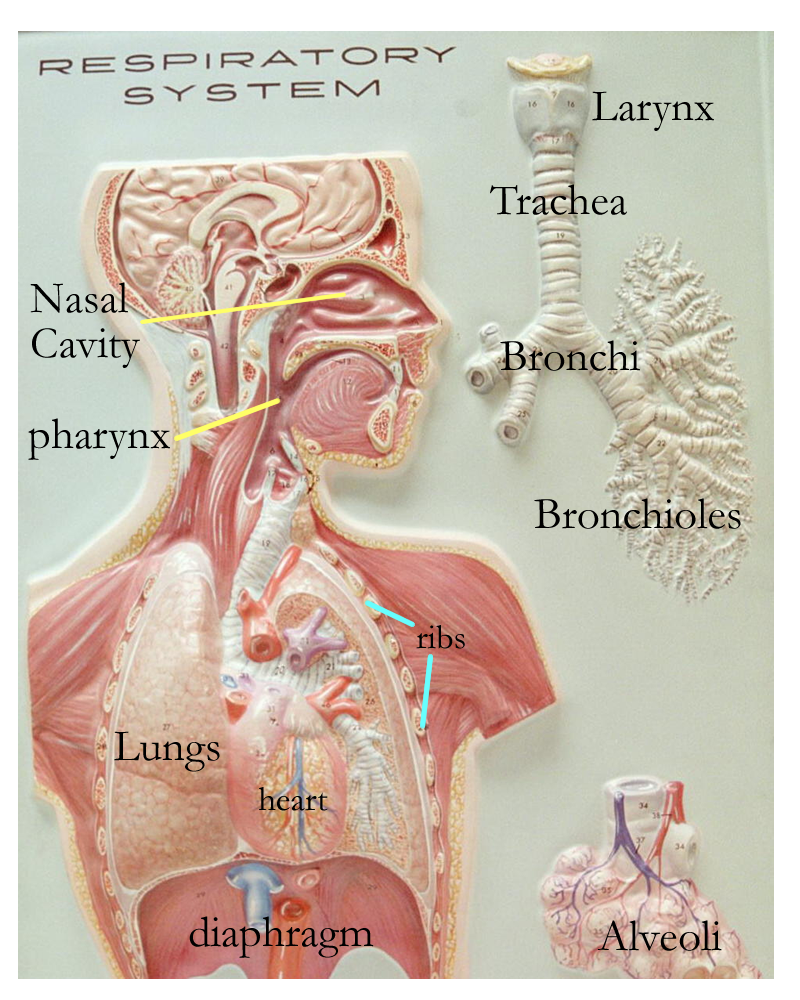
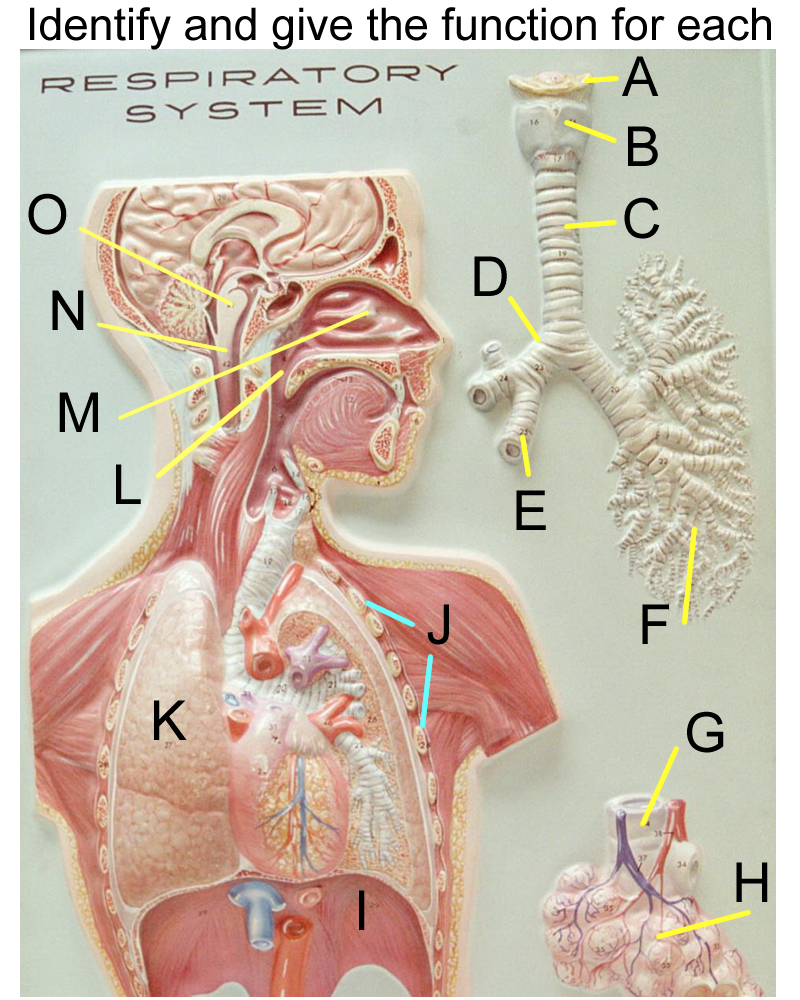
Wall Mount of Respiratory System
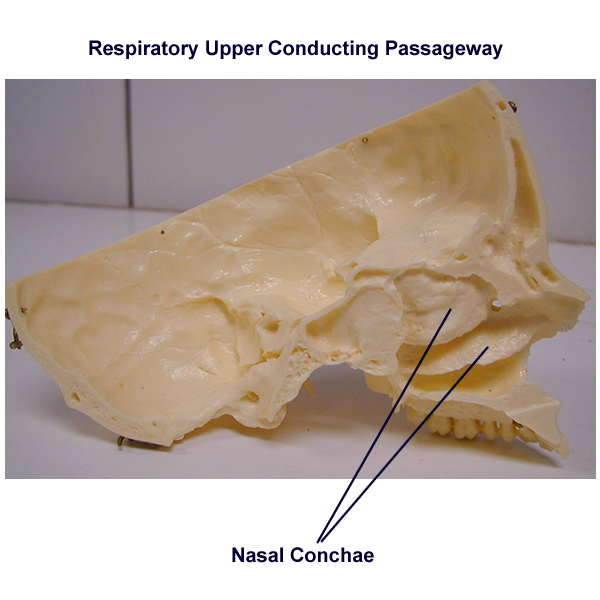
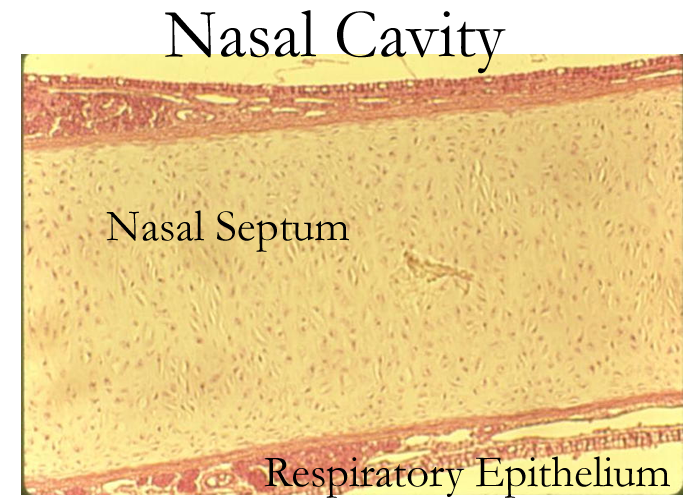
Nasal Cavity
The nasal cavity is formed by the bones of the skull and lined with a mucus membrane called the respiratory epithelium.
Components of the nasal cavity are:
External and Internal nares
Vestibule
Cranial bones: Ethmoid, Sphenoid, Frontal
Facial Bones: Nasal, Vomer, Maxillary, Palantine, Inferior nasal conchae
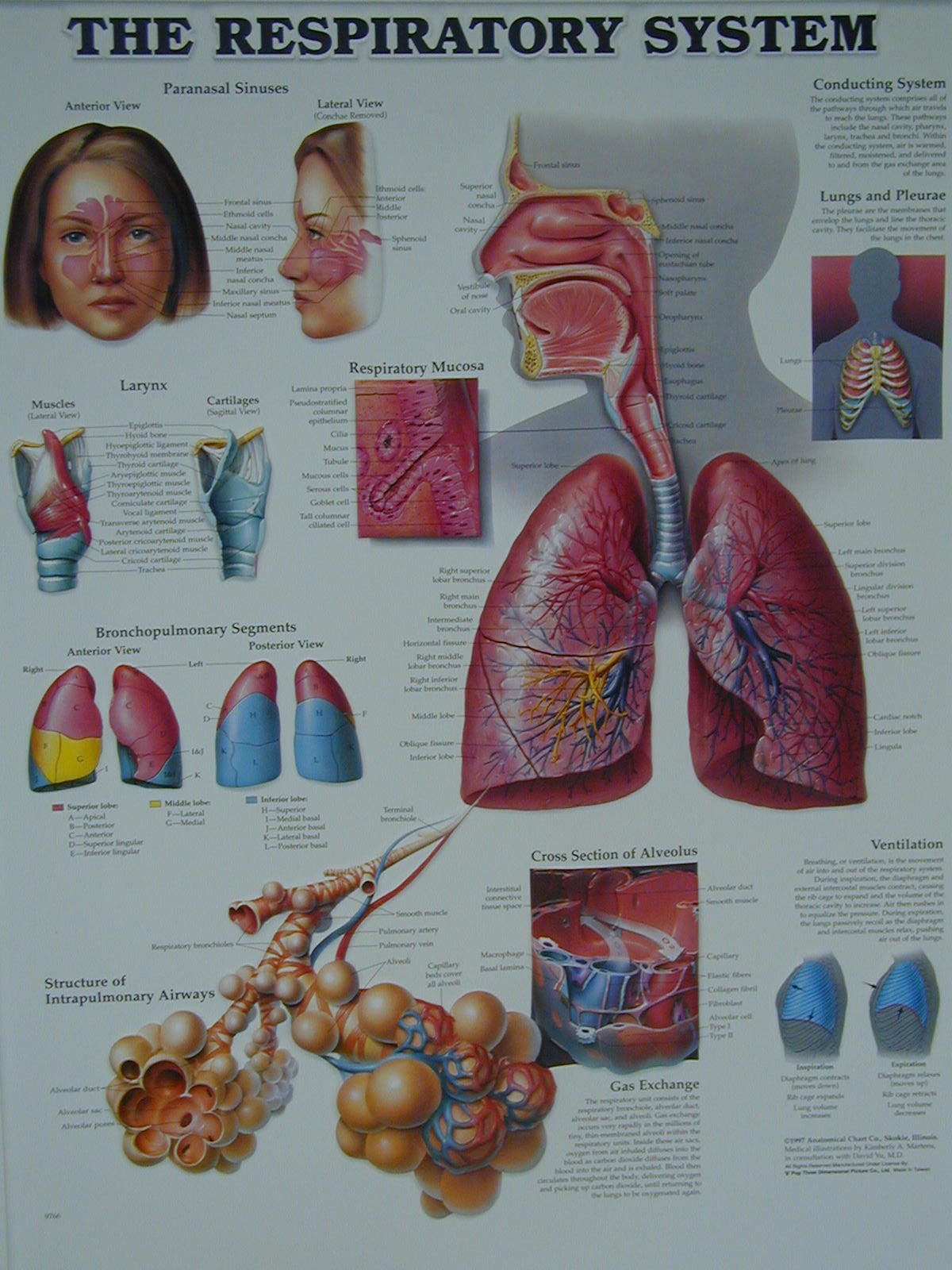
Paranasal Sinuses: Located in the Frontal, Ethmoid, Sphenoid, & Maxillary bones
Nasal Septum: Perpendicular plate of the Ethmoid, Vomer, and Hyaline cartilage
Nasal turbonates or conchae with narrow passageways called meatuses
Functions of the nasal cavity relate to the linings found in the nasal cavity.
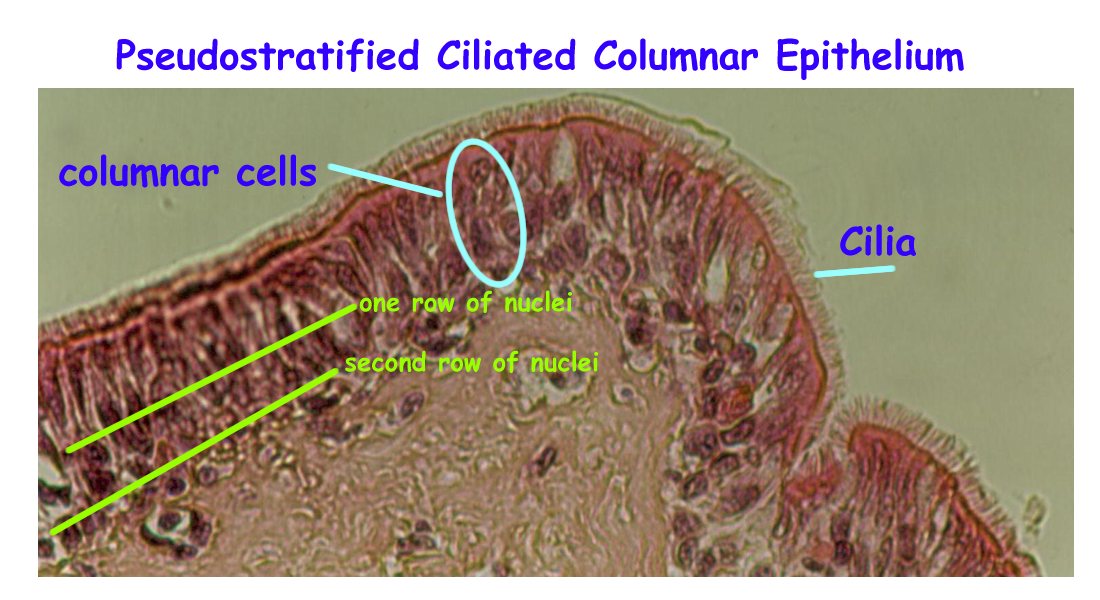
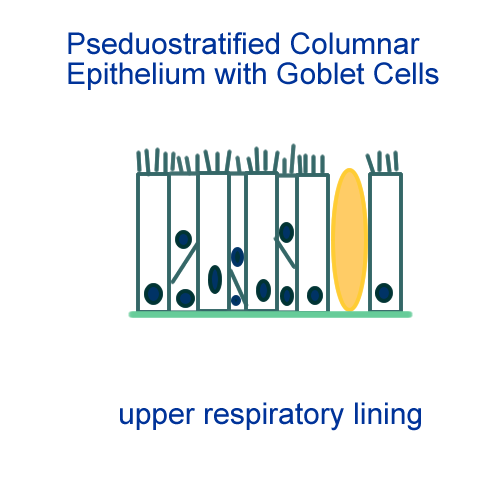
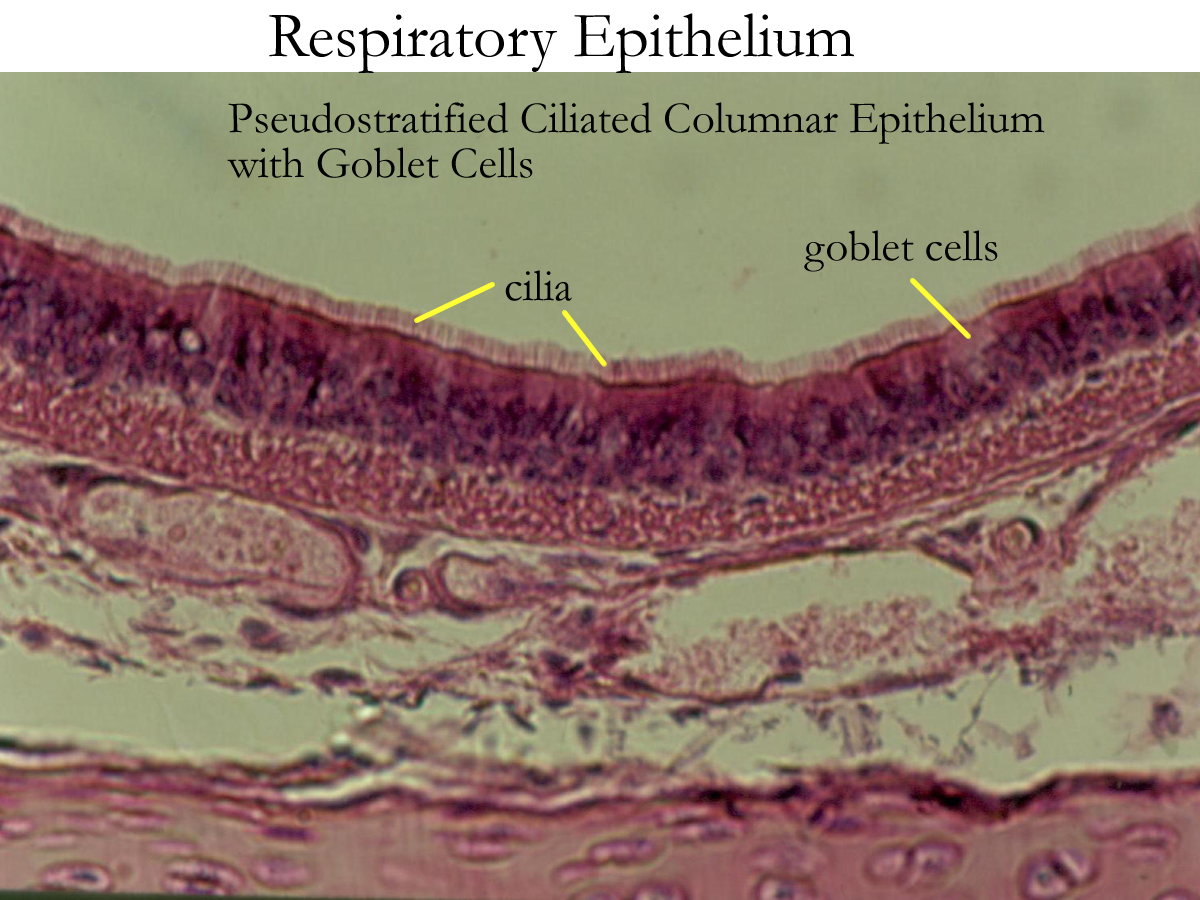
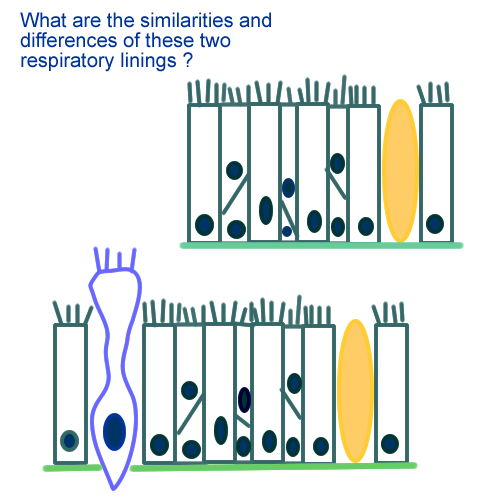
Respiratory epithelium = Pseudostratified columnar with goblet cells
Covers the structures in the nasal cavity
and functions to warm, filter, and moisten (humidify) incoming air
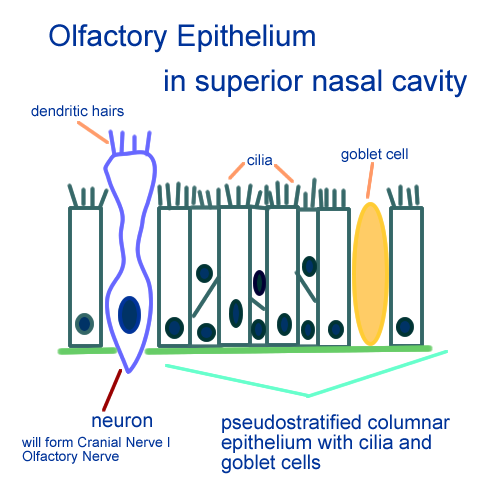
Olfactory epithelium= modified bipolar neuron and supporting cells
associated with the respiratory epithelium in the superior meatus that
functions in Olfaction. (See special senses)
Drawing of Respiratory epithelium
Pharynx
The pharynx is a muscular tube that forms a common passageway for food and air.
A more common name for this region is the throat.
It is lined with stratified squamous epithelium and divided into three regions:
Nasopharynx behind the nasal cavity
Contains pharyngeal tonsils and tubal tonsils
Functions in air conduction and immune defenses
The soft palate or uvula closes to prevent food from entering the nasal cavity.
Eustachian tube
opens from the middle ear to allow equalization
of air pressures at the ear drum
Oropharynx behind the oral cavity
Contains the palatine arches, palatine tonsils and lingual tonsils
Functions to provide air and food passageway and immune
defenses. Aids in swallowing
Laryngopharynx behind the larynx
Functions to connect to either the esophagus posteriorly or the trachea anteriorly. Aids in the swallowing reflex.
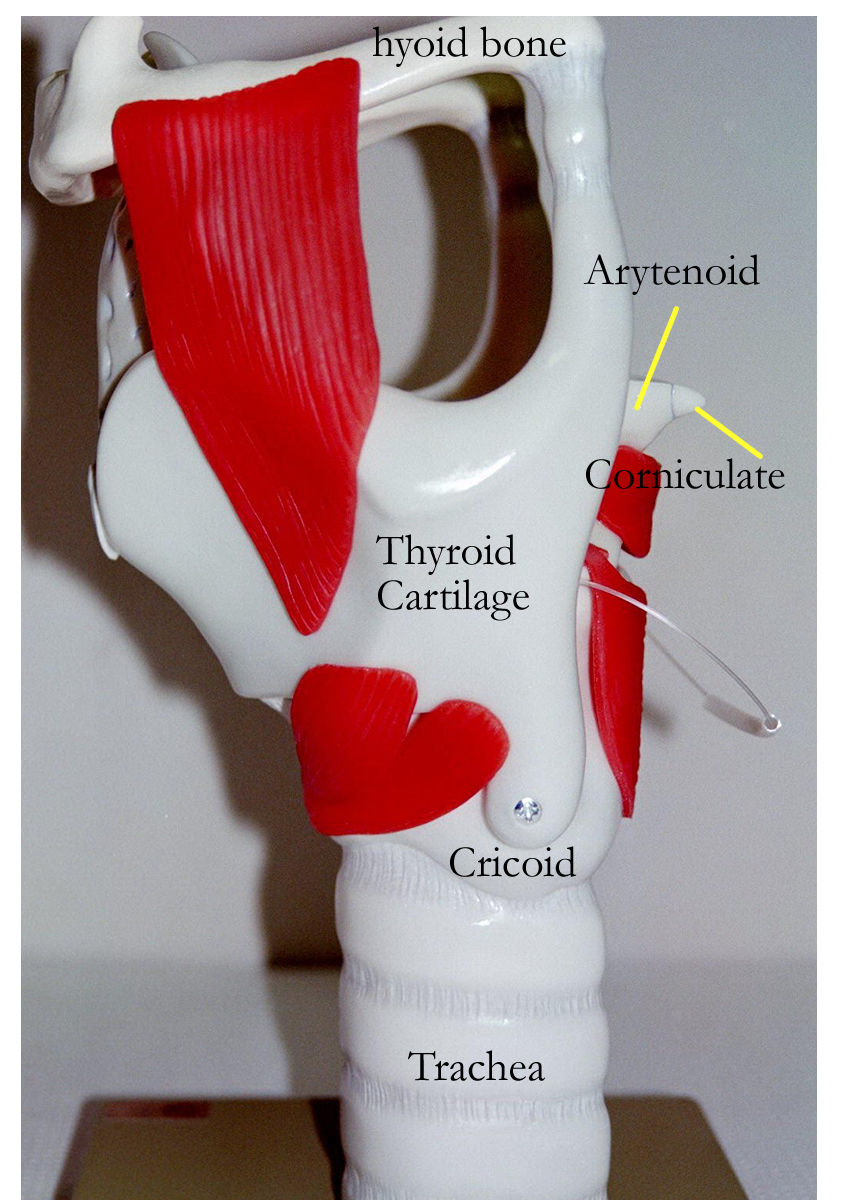
Larynx
The larynx is a cartilage tube that connects the pharynx to the trachea. A common name used for this region is the voice box. Most of the cartilage structures form a ring to create a patent (open) passageway. The cartilage is mainly hyaline and is covered primarily by respiratory epithelium.
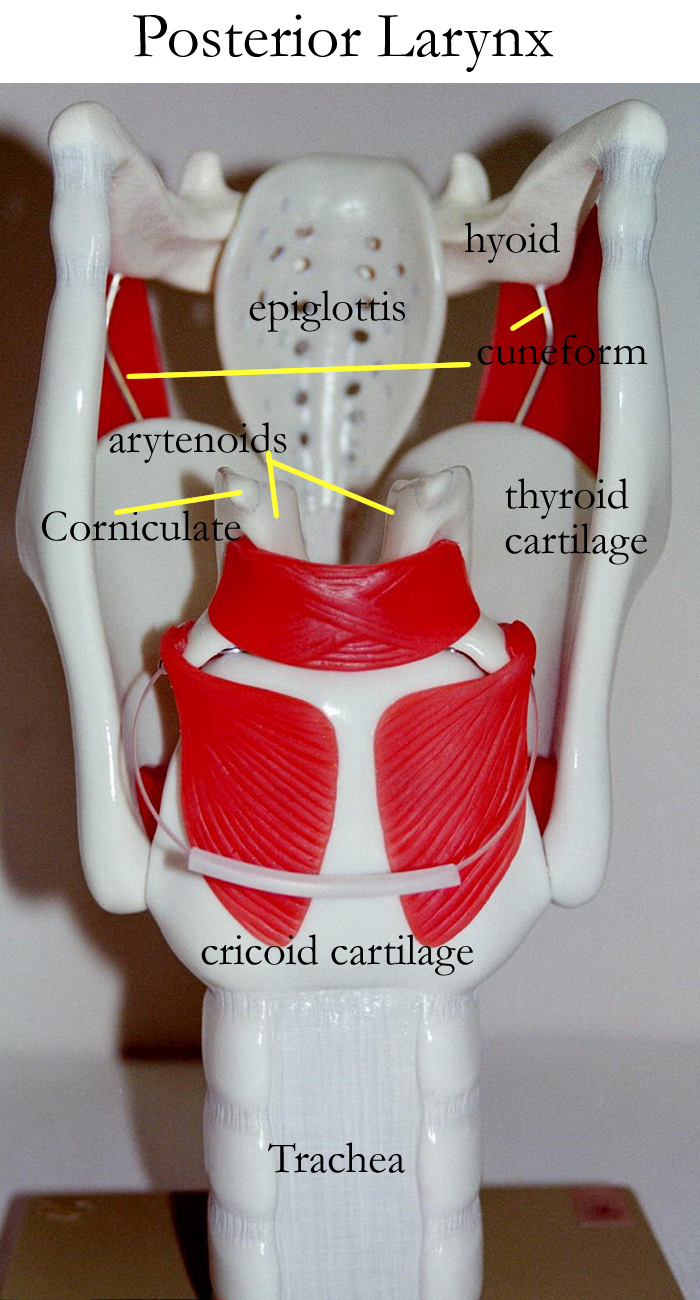
The laryngeal cartilages are:
Cricoid, corniculate, cuniform, arytenoid, thyroid, and the epiglottis
Some cartilages are paired such as the corniculate, cuniform, and arytenoids.
Others are singular such as the cricoid, thyroid, and epiglottal cartilages.
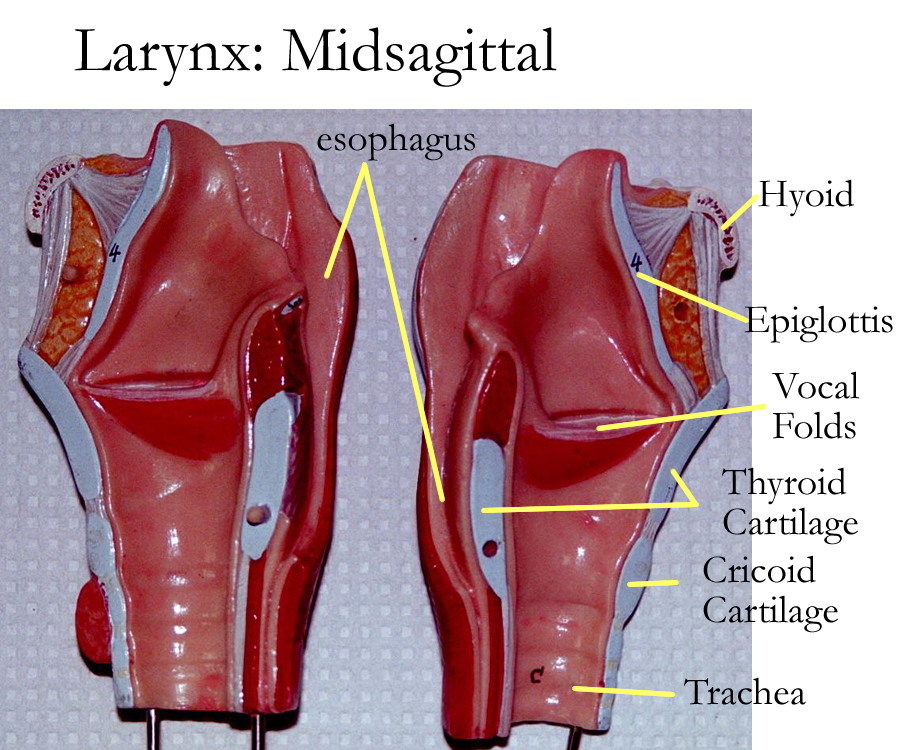
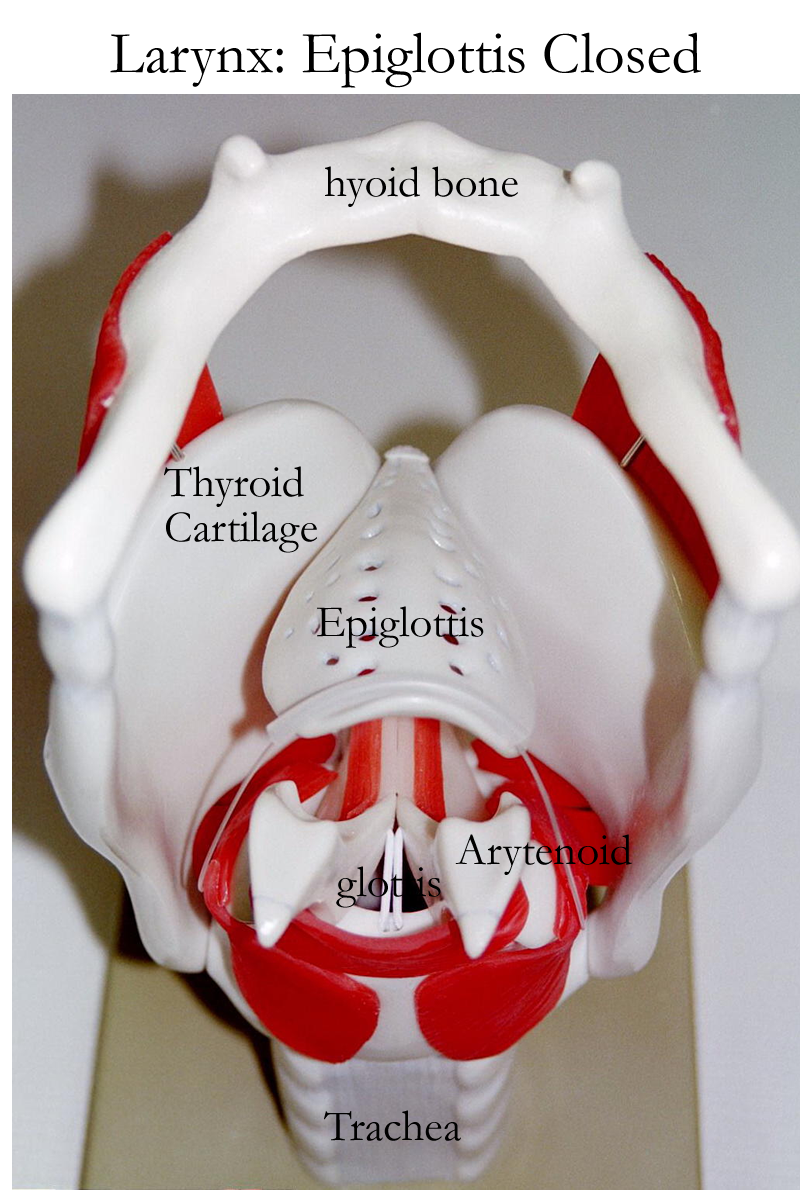
The epiglottis is a singular, tear drop shaped, elastic cartilage and is covered in stratified squamous epithelium. When swallowing food, it functions to close off of the glottis or entry into the trachea to prevent food or liquids from entering into the conduction passageways of the lower respiratory tract and the lungs.
The thyroid and cricoid hyaline cartilages function to maintain an open air passageway.
The corniculate, cuneiform, and arytenoids function in vocalization by anchoring connective tissue vocal cords and folds. Intrinsic laryngeal muscles pull on the cords to create various pitches and air moving out of the respiratory tract allows for sound production. Extrinsic laryngeal muscles help move the larynx out of the way during the swallowing reflex.
Enlarged Larynx: Anterior, Lateral, Posterior
Epiglottis Movements: Open, Closed
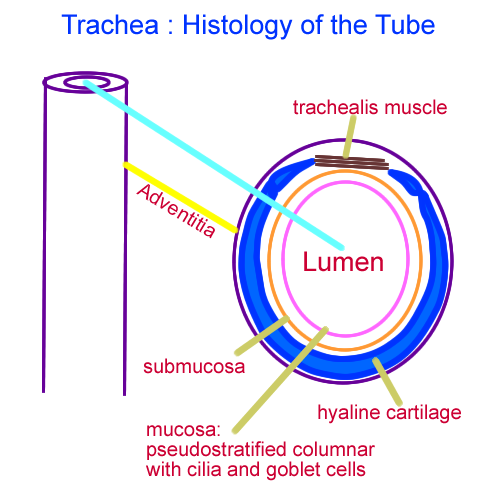
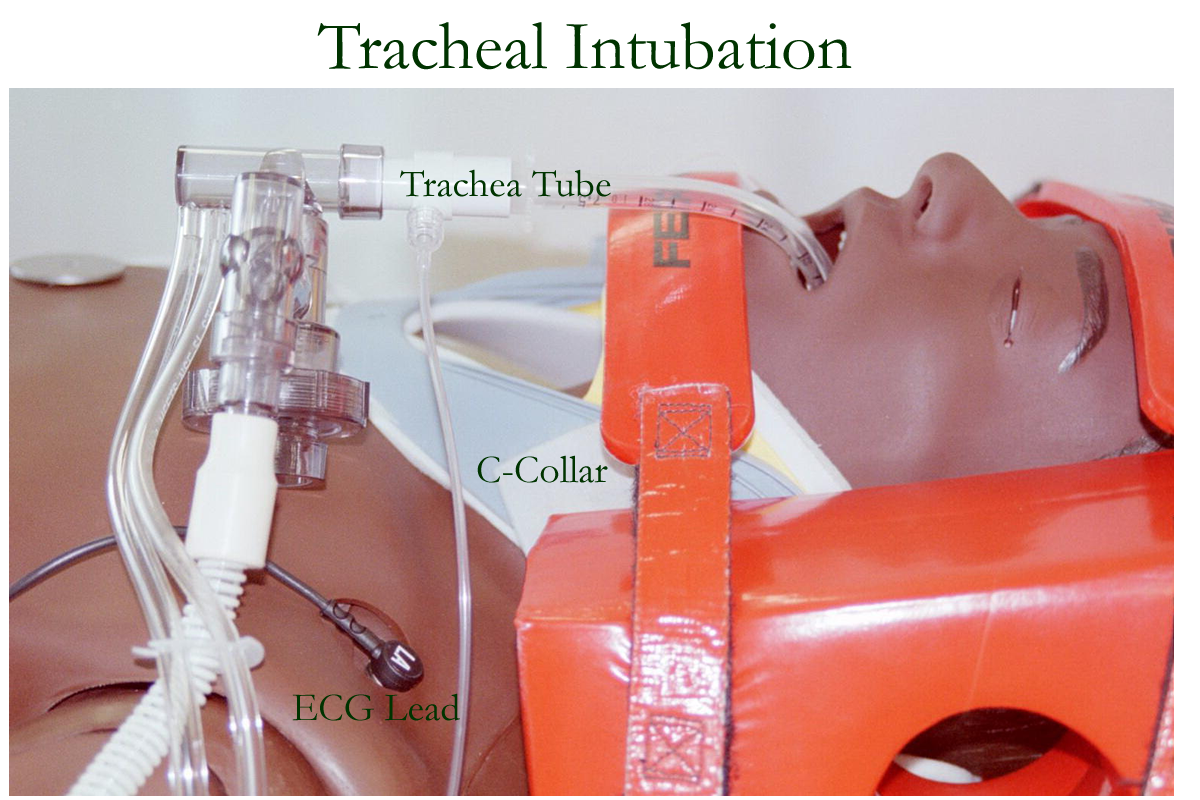
Trachea
The trachea is a 4.5 inch long cartilage tube found in the anterior neck region. It provides a passageway for air conduction and some filtration. A common name used for this region is the windpipe.
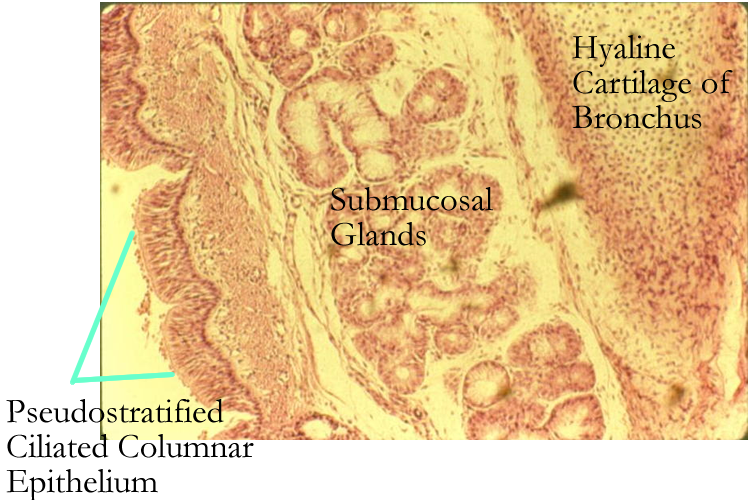
The lining or mucosa of the trachea is the respiratory epithelium: pseudostratified columnar with cilia and goblet cells. The goblet cells produce mucus that aids in trapping smaller substances not filtered in the nasal cavity. The cilia of the trachea beat upwards toward the mouth to help remove the filtered substances out by swallowing or coughing.
Under the tracheal mucosal lining are incomplete “C” or “U” shaped hyaline cartilage rings. These rings help keep the trachea open and the trachealis muscle that completes the tubular circle to allow for esophageal expansion when food moves through the esophagus.
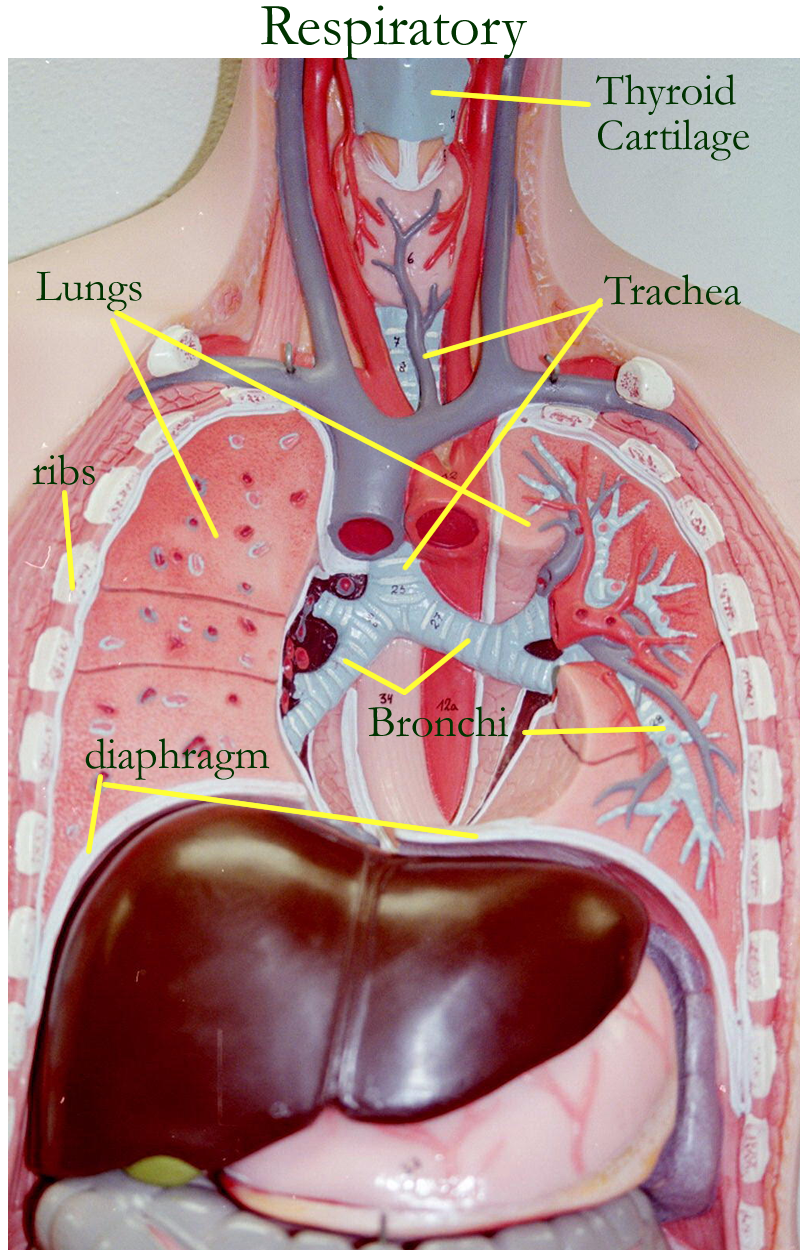
The last tracheal cartilage ring termed the carina is fused and forms a reference for radiography and bronchoscopy. The trachea ends when it divides into the right and left bronchus.
Bronchial Tree and Bronchioles
The bronchi begin as the trachea divides into right and left lower air conducting passageways. The bronchi are named according their divisions or generations. The first division creates the right and left primary bronchi. Each primary bronchus enters their respective lung. The incomplete cartilage rings and respiratory epithelial lings are found in these areas.
Upon entering the lungs, the primary bronchi divide into secondary bronchi or lobar bronchi that enter each respective lung lobe: two lobar bronchi on the left and three lobar bronchi on the right. Secondary bronchi divide into smaller tertiary bronchi and the branches continue for about 25 divisions or generations to create the bronchial tree.
As the bronchi get smaller, the cartilage ring breaks into cartilage plates and the respiratory lining changes from pseudostratitifed to simple columnar and then to simple cuboidal. The walls are held open by the cartilage, but the filtration mechanism is lost as the lining changes. At this point, the function is to conduct air into the smaller passageways. Filtration and defense are left to macrophages in the air sacs.
Smaller bronchi called bronchioles do not contain any hyaline cartilage in their walls.
The cartilage is replaced by smooth muscle in a circular plane which can constrict or narrow these air way passages. The final branches of this section are termed terminal bronchioles.
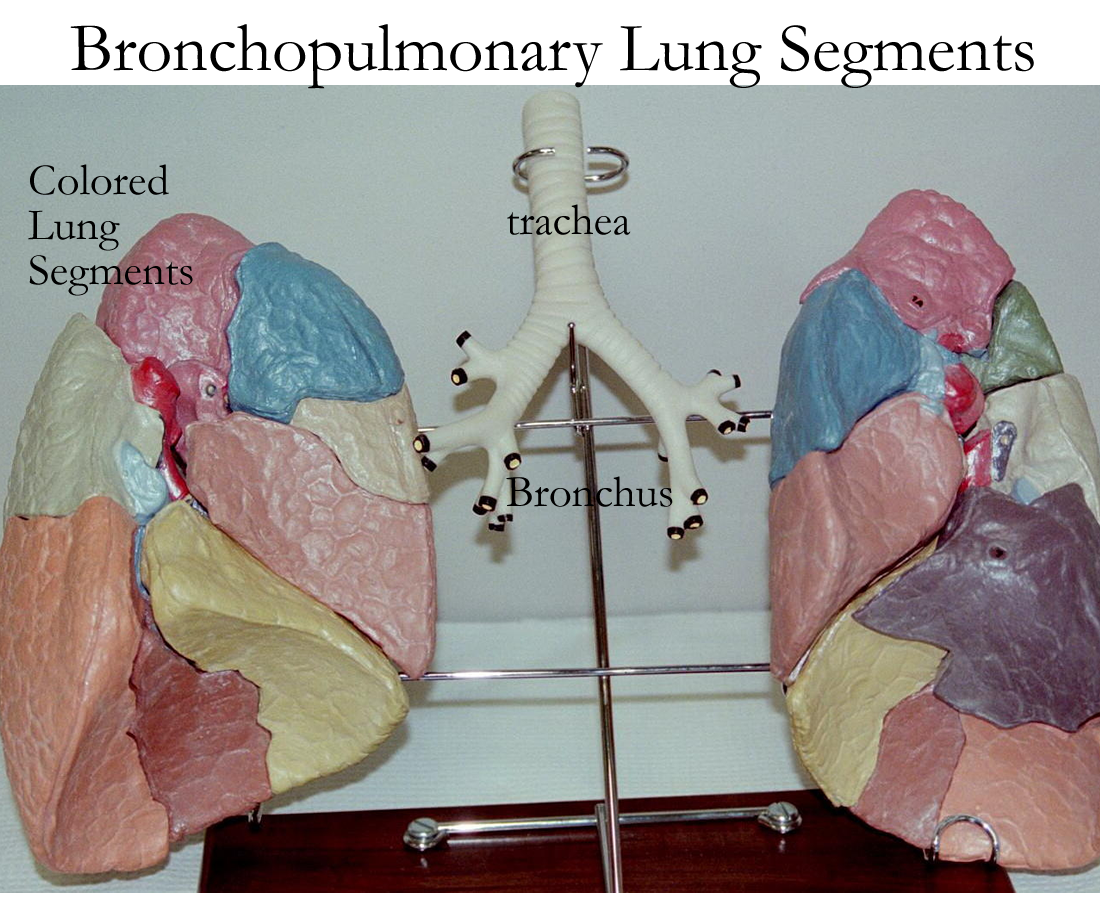
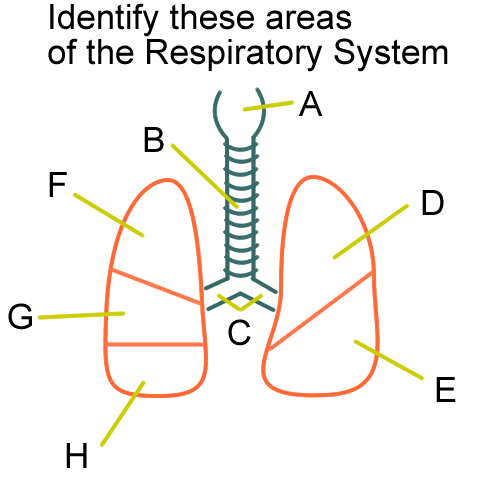
Bronchopulmonary Lung Segments
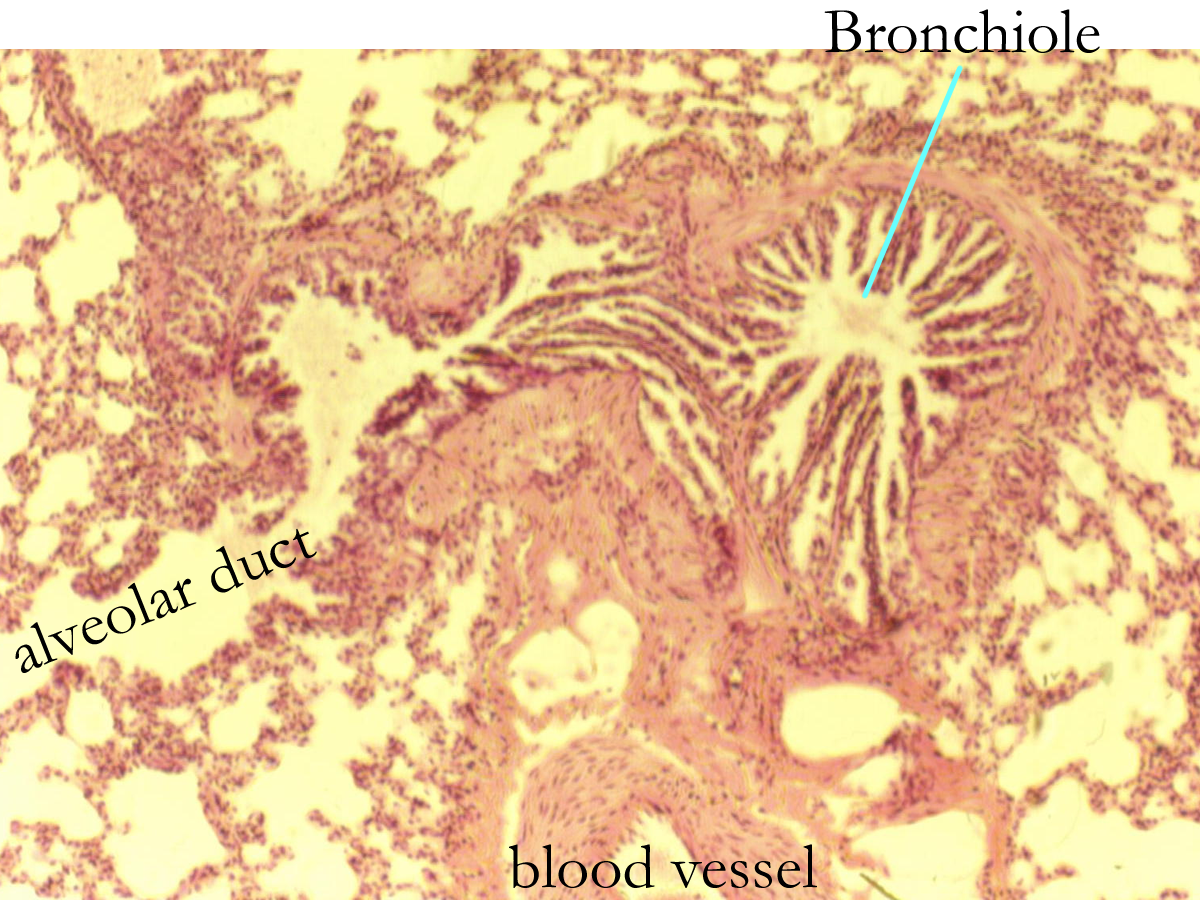
Lung histology with bronchioles
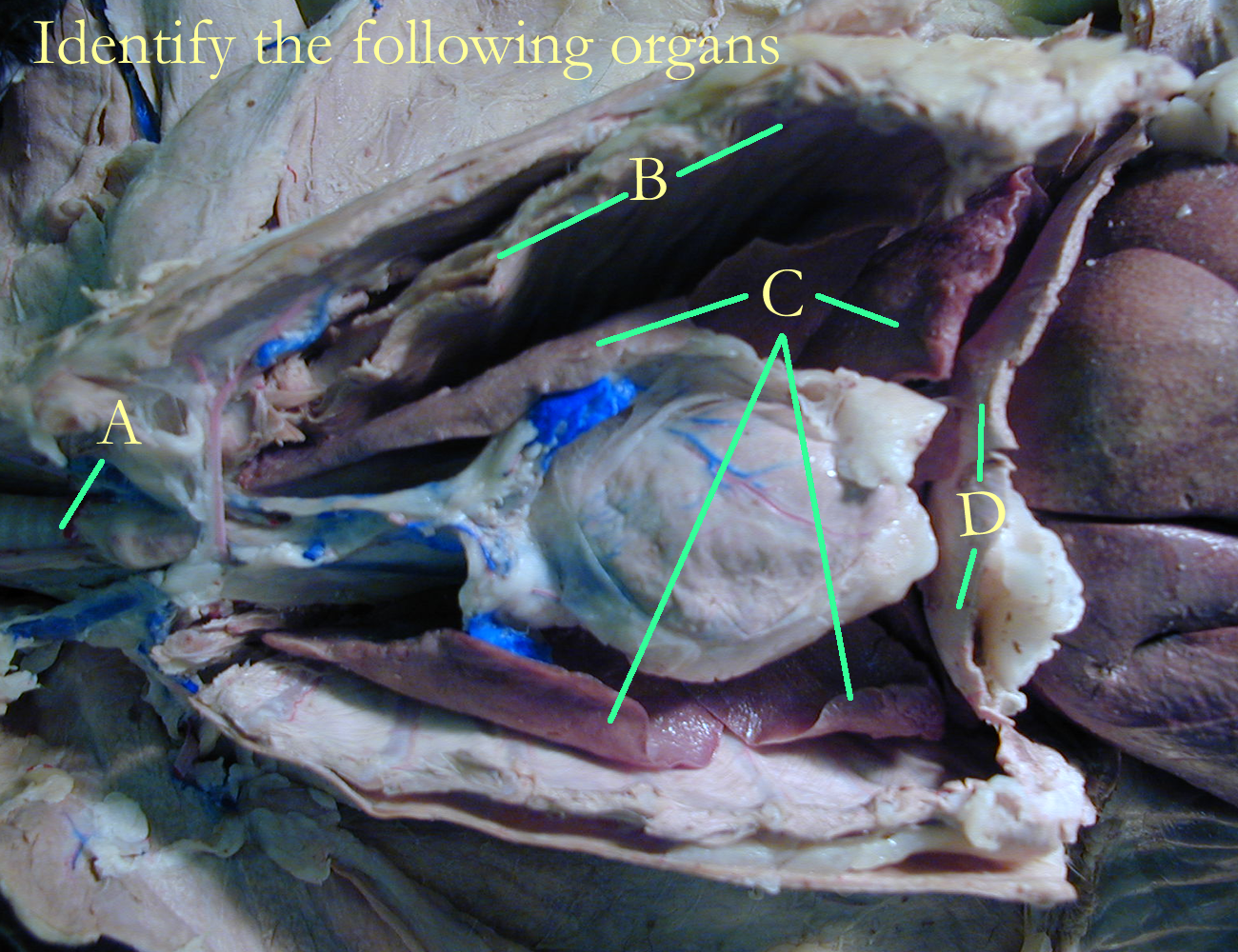
Lungs and alveoli
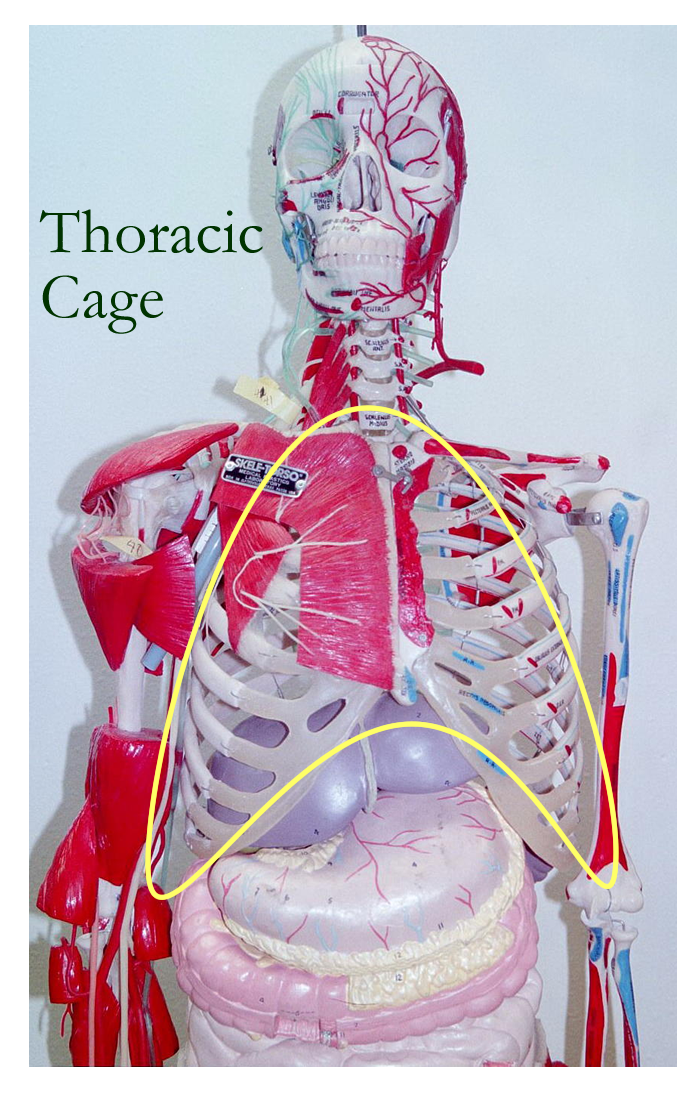
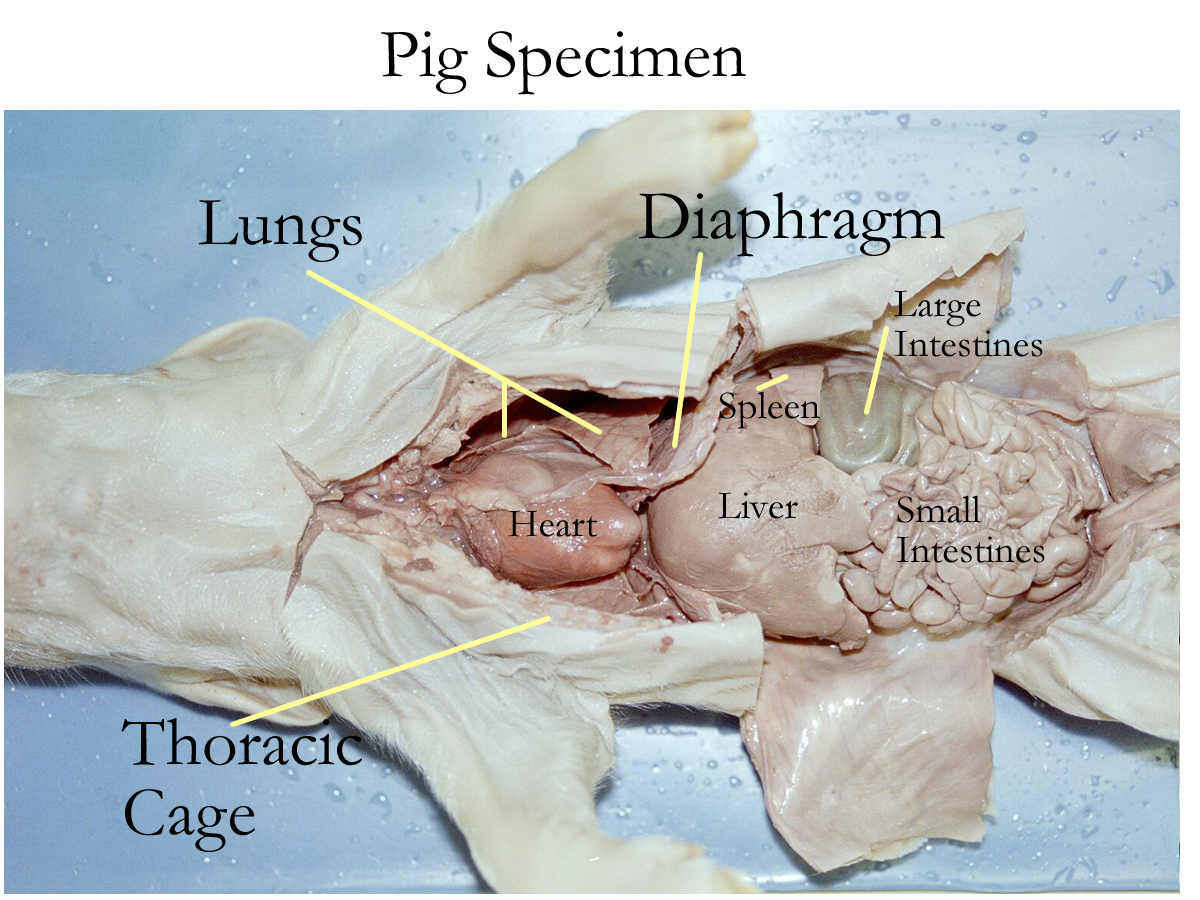
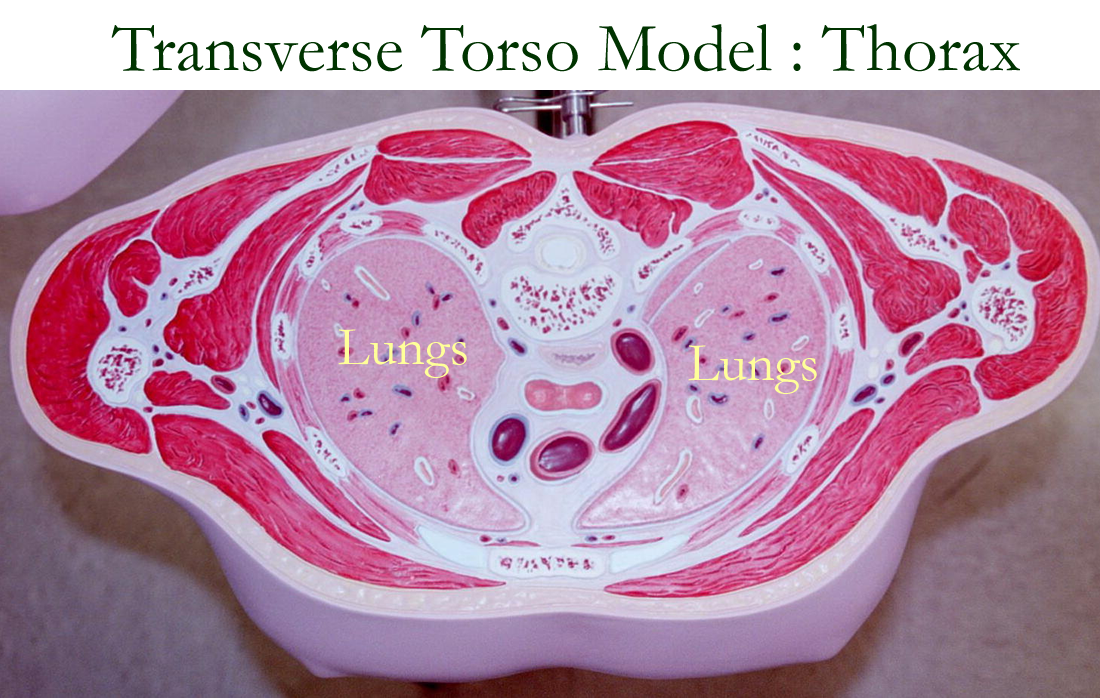
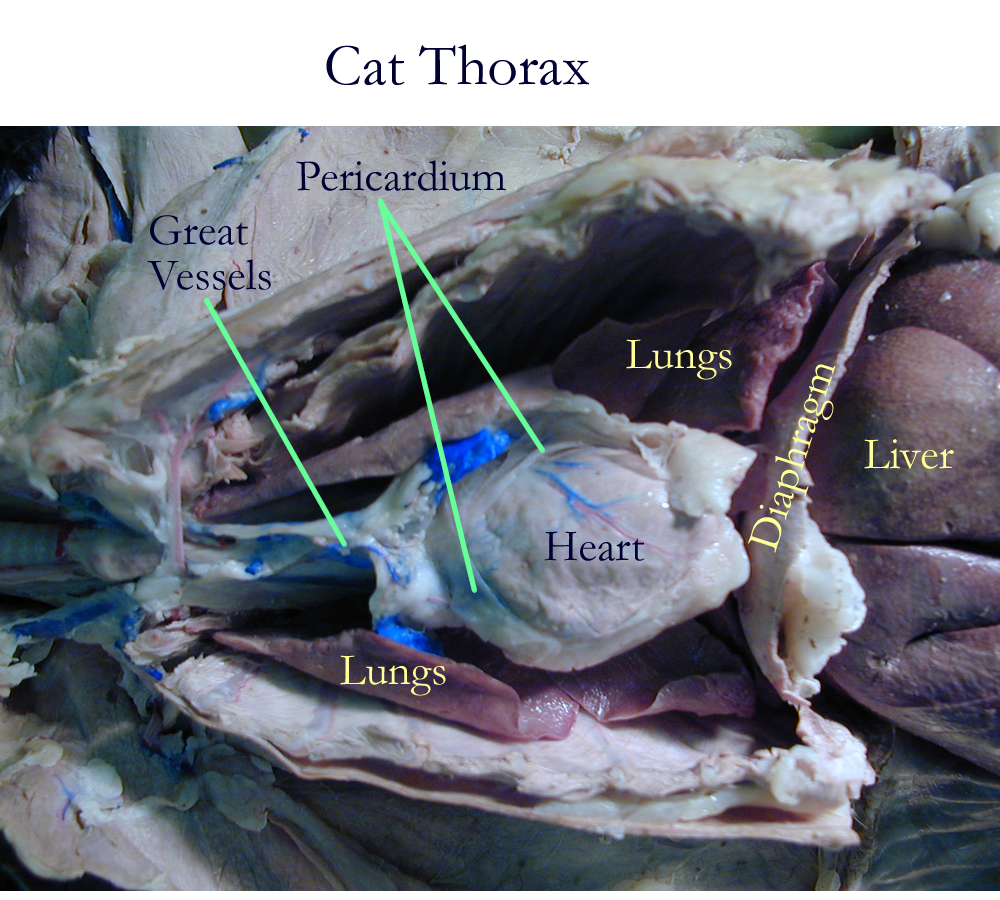
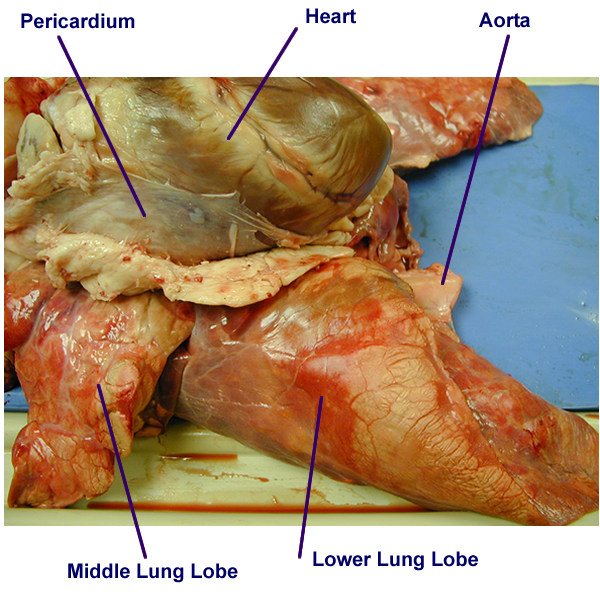
The lungs are located in the thoracic cavity, protected by the thoracic cage formed by the ribs, sternum, and thoracic vertebrae. The lungs are covered by a serous membrane known as the pleura. The pleural sac has an outer parietal portion that lines the chest wall and the inner visceral portion that is integrated with the lung tissue itself. The lung pleura not only helps decrease friction in movement, it helps in pulmonary ventilation to keep the lungs slightly expanded.
Their gross anatomy consists of paired right and left organs with a broad base that sits on the skeletal muscle diaphragm and pointed apex that extends above the clavicle. On the medial surface there is a hilus or indentation where the primary bronchi and associated blood vessels enter and leave.
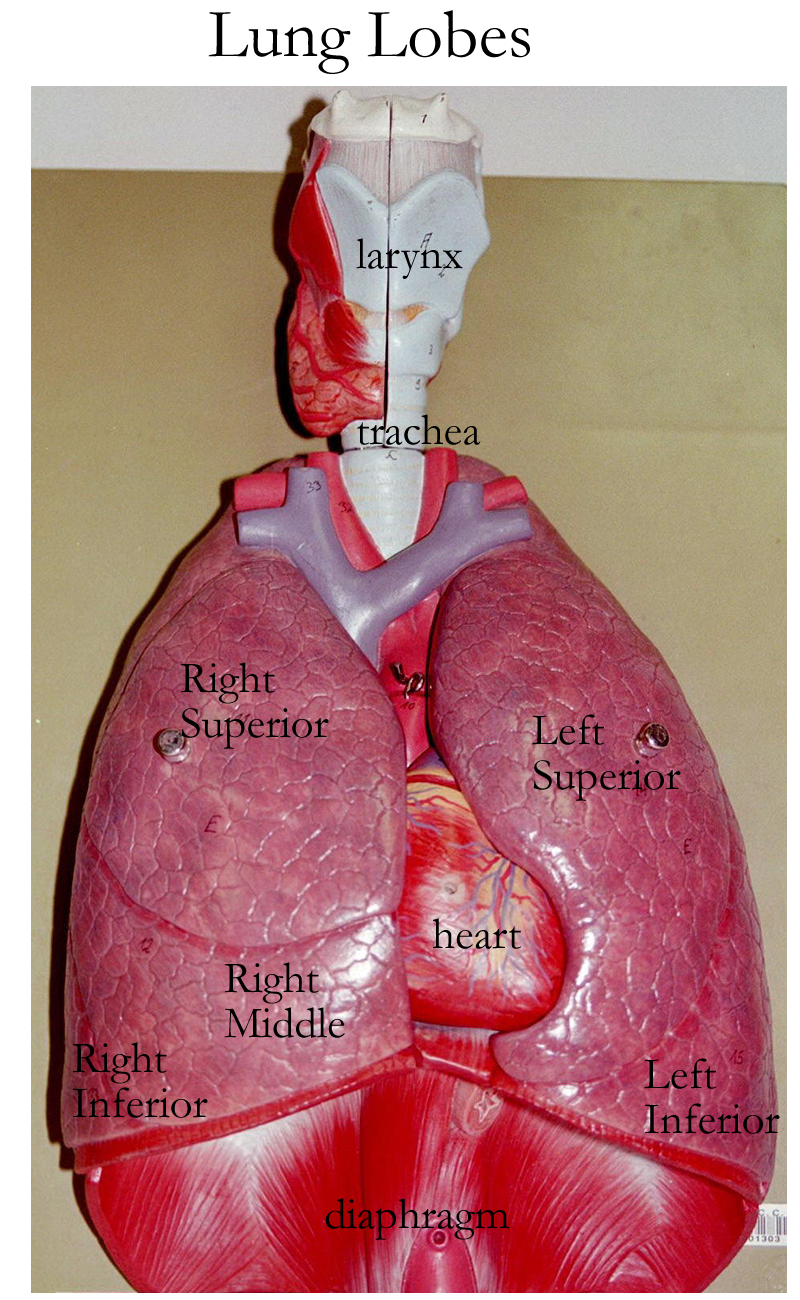
The lungs are divided into lobes created by fissures of connective tissue. The left lung is divided by a horizontal fissure to create the superior and inferior lung lobes. The right lung is divided by a horizontal and oblique fissure to create the superior, middle, and inferior lung lobes. Each lung lobe is further divided by connective tissue to create lobules that correspond to a bronchopulmonary segment.
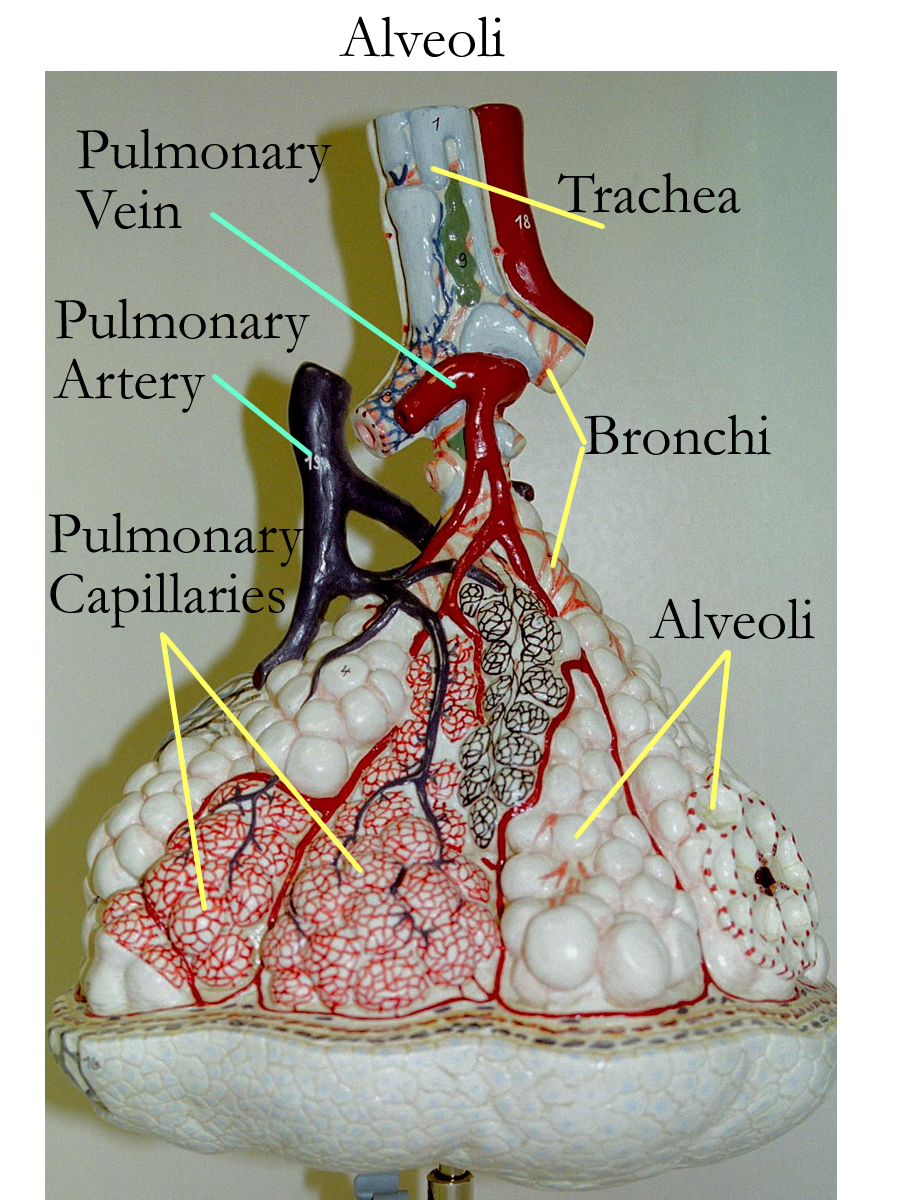
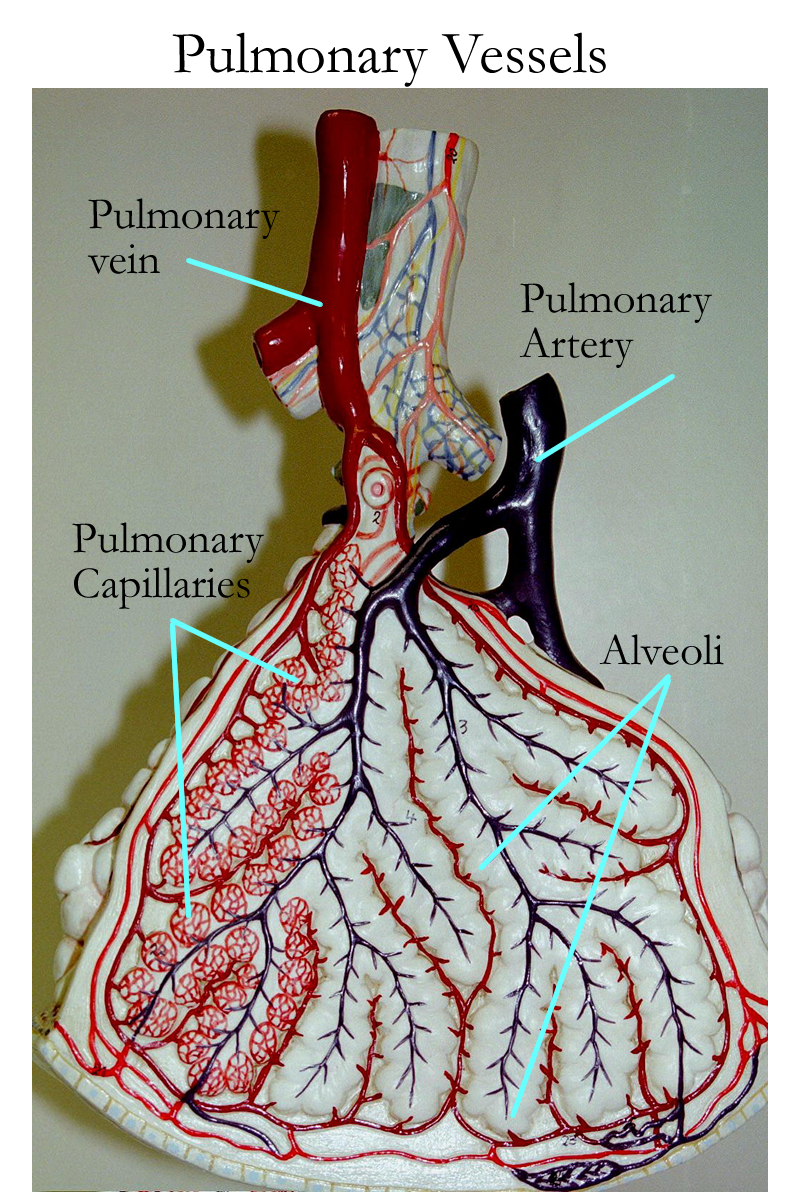
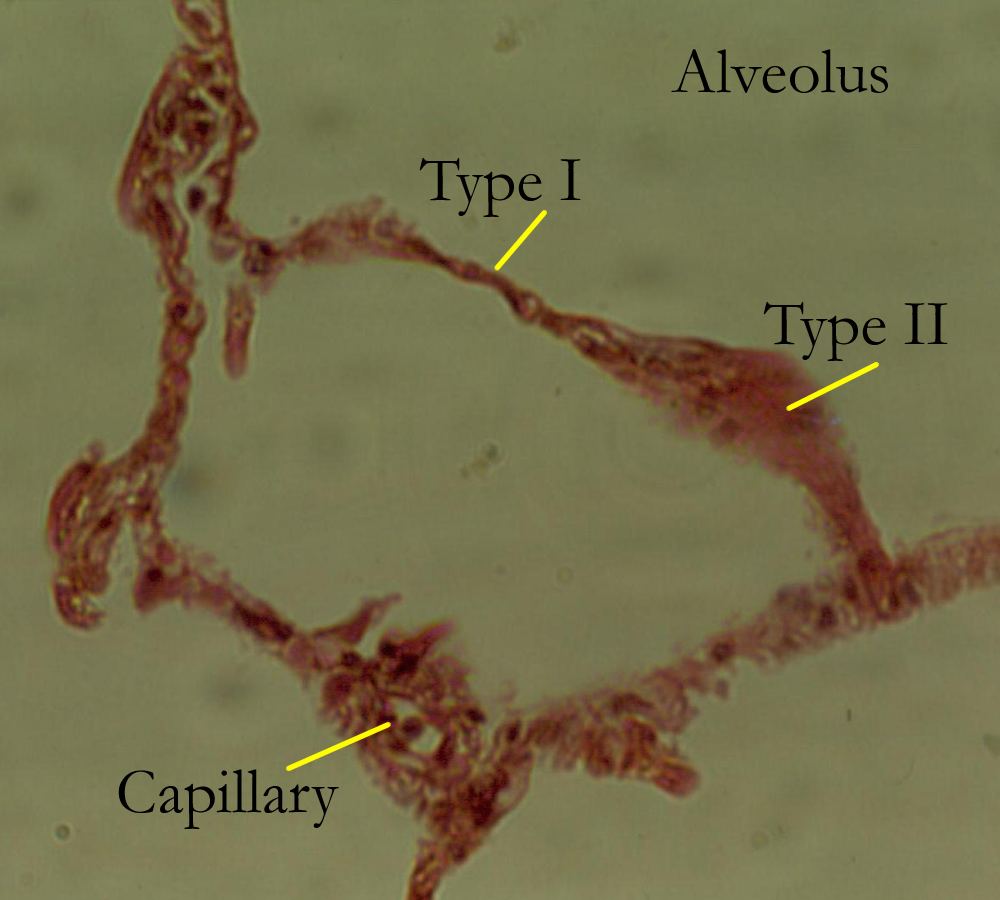
The lungs are composed of elastic connective tissue and air sacs called alveoli. The terminal bronchioles continue to divide into alveolar ducts that lead to expansions in their wall known as an alveolus. The alveolus is a simple squamous lined sac that functions in gas exchange. It is part of the respiratory membrane when combined with the pulmonary capillary blood supply. There are also other cells in the alveolus besides the Type I alveolar (simple squamous) cell. Type II (septal) alveolar cells are cuboidal and function to secrete a lipoprotein called surfactant that decreases water surface tension in order to prevent alveolar collapse. Alveolar macrophages are also present and aid in immune defenses.
The negative intrapleural pressures created by the pleura on the lungs also help to overcome the elastic tendency of the lungs to collapse the air sacs.
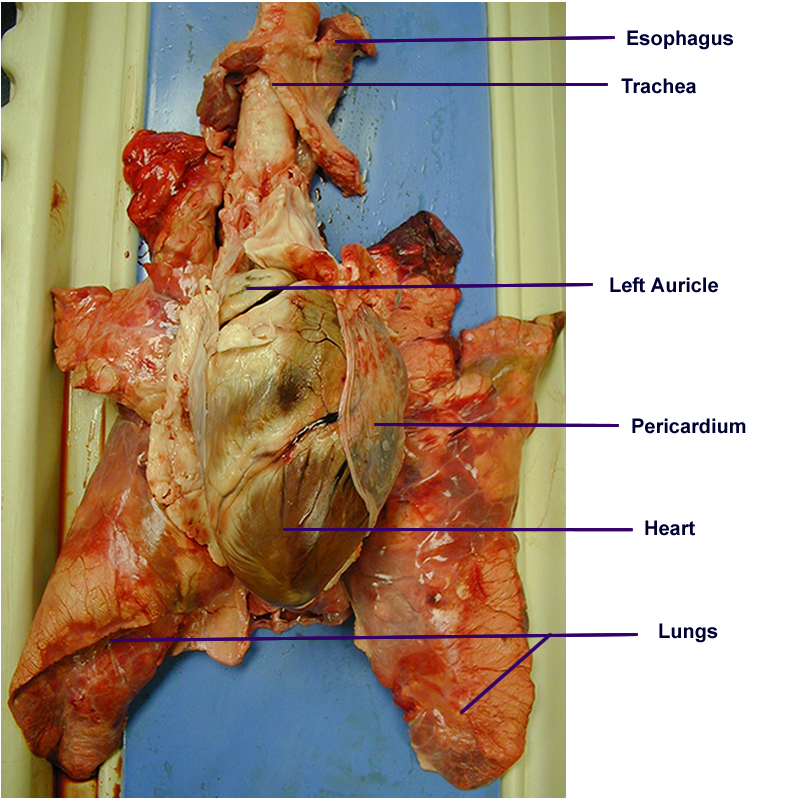
Body Torso : Anterior, Interior
Specimens: cat, pig, pig pluck
Respiratory Physiology
As defined earlier, respiration is the process of gas exchange and has four phases that are continuous with each other. The four respiratory phases are pulmonary ventilation, external respiration, internal respiration, and cellular respiration.
Pulmonary Ventilation
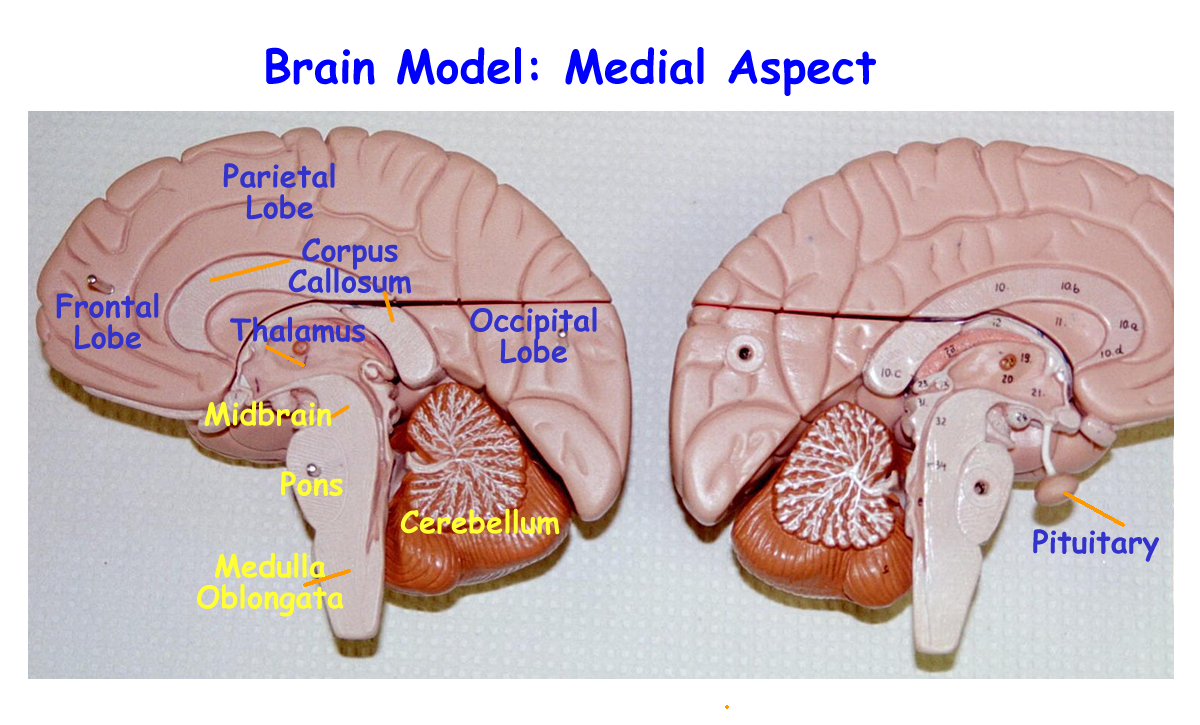
Ventilation is the movement of air in and out of the respiratory tract. The two processes of ventilation are inspiration and expiration and are primarily controlled via the brainstem regions of the medulla oblongata and the pons. Inspiration begins with contraction of the primary skeletal muscle of respiration, the diaphragm and the contraction of the external intercostals muscles.
The phrenic and intercostals nerves are used to signal the diaphragm and external intercostals, respectively. Shortening of these muscles allows for expansion of the chest cavity and the volume changes lead to pressure changes that allow air to move into the respiratory tract. Expiration occurs passively when the skeletal muscles relax. The chest cavity volume decreases, pressures increase inside and air flows outward from the tract.
Additional air can be moved in and out during forced inspiration and forced expiration. To breathe more air in or out requires activation of additional skeletal muscles. Forced inspiration requires muscles of the neck to be activated for contraction and forced expiration requires activation for contraction of the abdominal muscles.
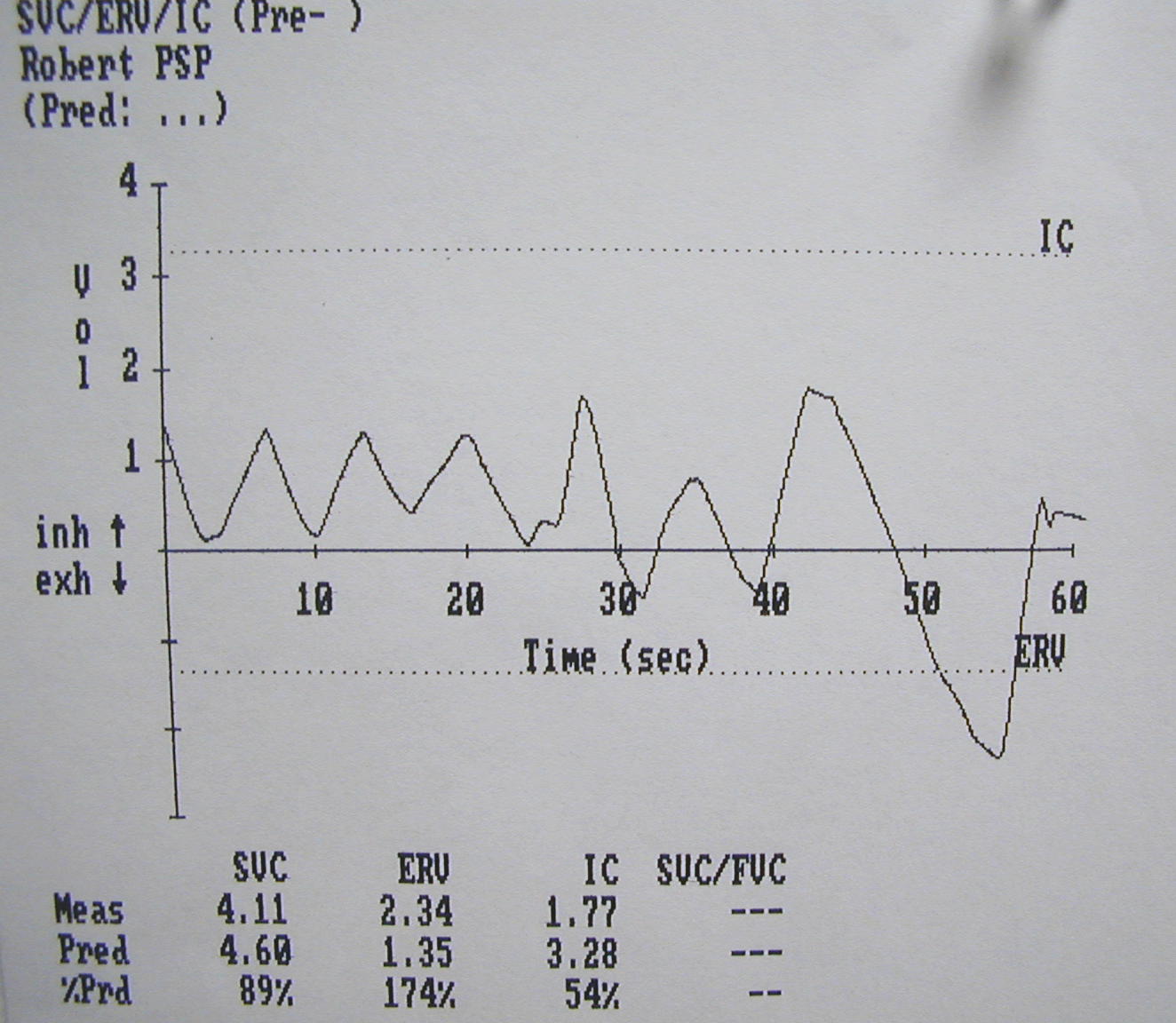
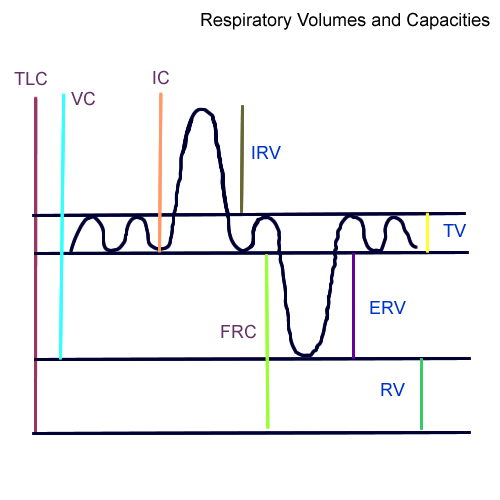
Ventilation can be monitored and tested. The volume of air that is moved can be measured by a spirometer. Two types of spirometers exist: wet and dry. The normal movement of air during a normal, quiet ventilation cycle is called tidal volume or TV.
Other volumes are inspiratory reserve volume (IRV), expiratory reserve volume (ERV), and residual volume (RV). The inspiratory and expiratory reserve volumes measure the amount of air that can be moved over and above a normal TV. Residual volume is the air that remains in the respiratory tract when the ventilation cycle ends.
The respiratory ventilation volumes can be added together to create respiratory capacities. A commonly calculated capacity is the vital capacity, VC, and is the sum of IRV + TV + ERV. All the respiratory volumes added together equal the total lung capacity, TLC.
Other tests performed using pulmonary ventilation are respiratory rate or number of breaths per minute and respiratory sounds or sounds heard through a stethoscope when air moves in and out of the respiratory tract. Percussion or tapping on the chest wall while listening to air movement can also be done and is used to detect fluid levels if present.
Respiratory volume printouts: TV/ERV #1, TV/ERV #2, Pulmonary Function
Respiratory Volumes and Capacities Drawing
Ventilator : Bedside, Adult, Pediatric, Bipap
****************************************************************************************
External Respiration
Once the air is in the alveolus, the exchange across the capillary-alveolar or respiratory membrane occurs. Gases move passively by diffusion and the gradient needed is created by each gases partial pressure and solubility. Though the gases that are primarily exchanged are O2 and CO2, the air we breathe also contains nitrogen and water vapor.
Each percentage of gas reflects its part of the whole pressure or partial pressure. All the gases in air will contribute a total pressure of 760 mmHg at sea level.
Partial pressures are written as P (partial pressure) then the symbol of the gas referenced.
Nitrogen 78.6% of 760 mm Hg = P N2 is 597 mmHg
Oxygen 20.9% of 760 mm Hg = P O2 is 159 mm Hg
Carbon Dioxide .04% of 760 mm Hg = P CO2 is .3 mmHg
Water vapor .46% of 760 mm Hg = P H20 vapor is 3.7 mmHg
As the gases come into the respiratory tract, they are warmed, filtered and humidified. They will then mix with residual gases of previous ventilation cycles. By the time the gases enter the alveoli, the old and new mixture creates a PO2 of 100 mmHg and a P CO2 of 40 mmHg. Blood returning from the body tissues and entering the pulmonary capillaries has a P O2 of 40 mm Hg and the P CO2 is 45 mmHg.
Due to the pressure difference across the respiratory membrane, gases flow down their concentration and pressure gradients. Therefore the alveolar O2 at 100 mmHG enters the pulmonary capillaries which have a lower PO2 of 40 mm Hg until equilibrium occurs at a P O2 of 100mmHg. The blood P C02 at 45 mmHg enters the alveoli which has a PCO2 of 40 mmHg until equilibrium is reached at a P CO2 of 45 mmHg.
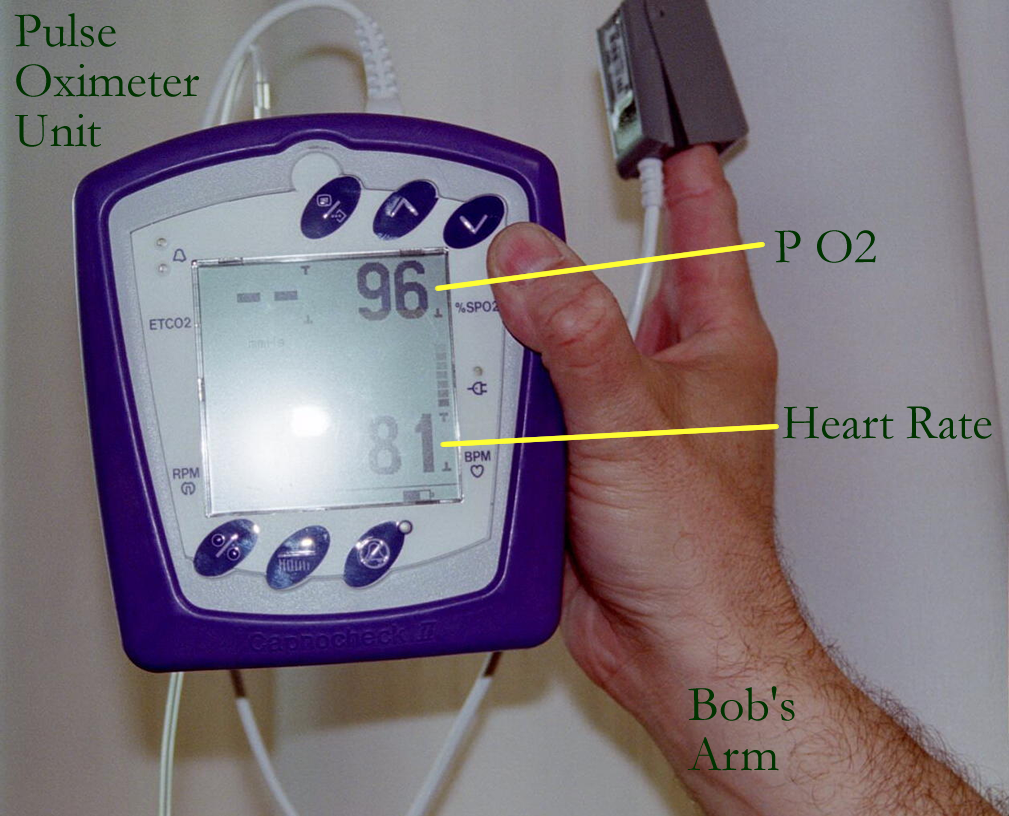
Blood leaving the lungs to be returned via the pulmonary arteries to the left side of the heart now has a P O2 of 100 mmHg and a P C02 of 40 mmHg. Blood that was brought to the lungs was said to be “deoxygenated” with a PO2 of 40 mmHg, while the blood returning from the lungs is said to be “oxygenated” with a PO2 of 100 mmHg. Measurement of this phase of respiration uses a pulse oximeter for an indirect reading and blood gases by drawing blood from an artery for direct readings.
Blood gas values: PCO2 = 35 mmHg - 45 mmHg
PO2 = 90 mmHG
****************************************************************************************
Internal Respiration
Internal respiration involves gas transport in the blood to the tissues.
Oxygen is transported one of two ways. The majority (98%) of the O2 is bound to the iron in the hemoglobin molecules contained in the RBCs. The rest of the O2 is transported as dissolved O2 gas in the plasma.
Carbon dioxide is transported one of three ways. The majority of the CO2 is transported as bicarbonate ion(HCO3-). A smaller amount (25%) is transported as CO2 on the globin of hemoglobin in the RBCs. The rest is transported as dissolved CO2 gas in the plasma.
The bicarbonate ion is created in the RBCs when CO2 in the presence of water and the carbonic enzyme first combines these molecules into a weak acid, carbonic acid, H2CO3. Since it is an acid, it is a hydrogen ion donor and in the presence of the same enzyme, will create H+ + HCO3-. That is, a proton (H+) known as hydrogen ion and bicarbonate ion, HCO3- are formed. H+ will dramatically change the pH of the blood; therefore, the RBC hemoglobin proteins will bind or tie up H+ to prevent drastic blood pH changes. HCO3- can then enter the plasma and joins with Na+ to form Sodium Bicarbonate that can also act as a pH buffer for blood. This reaction takes place as the blood is returned to the heart. In the lungs, the reverse reaction occurs and HCO3- is transformed back to CO2 to be eliminated during the expiratory phase of pulmonary ventilation.
In summary, O2 and CO2 are delivered to the tissues via gas transport mechanisms.
The tissues use the O2 in aerobic cellular respiration and more CO2 is created. Gases are returned to the respiratory system in the venous blood. Venous blood that is returned to the heart will be pumped to the lungs for gas exchange during the respiratory cycle.
Bohr effect: Increased temperature, increased PCO2, increased H+ or decreased pH cause the dissociation curve to shift down and to the right, enabling oxygen unloading. The change in these factors happens at the tissues, so that oxygen will be released from the iron of the hemoglobin. The reverse effect happens in the lungs as the curve shifts up and to the left to help oxygen load more readily on the hemoglobin for transport. This happens because there is a decrease in temperature, decrease in PCO2, decrease in H+ or increase in pH.
****************************************************************************************
Cellular Respiration
Cellular Respiration is the use of respiratory gases to aid in aerobic metabolism of nutrients, such as glucose and it’s by products. Certain parts of fats and some proteins can be converted to glucose metabolites and used in a glycolytic pathway known as glycolysis. More will be discussed in the digestive system under metabolism.
Factors that Affect Respiration
Peripheral Controls
Physical factors: talking, temperature, exercise
Emotional factors: scared, excited
Chemical factors: blood pH, O2, CO2
Central Controls
Brainstem: Medulla sets the respiratory rate at 15 breaths per minute
Pons adjusts respiratory rate to increase or decrease
Hypothalamus: long term control over brainstem respiratory functions
Cerebral cortex: conscious motor cortex control over skeletal muscle
Oxi- oxygen atel- imperfect
Bronch- windpipe -ectasis expansions
Laryng.o- larynx pharyng/o- pharynx
Pneum- lung, air nas/o- nose
Rhin/o- nose -stomy mouth like opening
-
pleur- rib, side pulm/o-, pulmon/o- lung
spirat/o- breathe spir/o- breath, air
-phonia sound glott/o- glottis
adenoid/o- adenoids alveol/o- alveolus
-capnia CO2 -osmia smell
-ptysis spitting eu- normal, good
lob/o- lobe phren/o- diaphragm, mind
tuber- swelling phlegm- burn, inflame
I. ID and FXN of respiratory tract organs
A. Models: Wall Mount, Green Base
II. Respiratory rate : Obtain a watch with a second hand and do the following experiments.
At rest: count your normal breaths per minute.
While talking for two minutes, have someone count the number of breaths you take.
After exercising for 5 minutes, count the number of breaths you take per minute.
Name two peripheral factors and two central areas that control breathing. Which one(s) are active in each of the activities:
breathing at rest
breathing while talking
breathing while exercising.
Now try holding your breath for as long as you can. Record the time. What changes happened in your body to overide your conscious control of breathing?
III. Breath sounds (stethoscope): Obtain a stethoscope and listen to breath sounds on yourself and another person. Explain the sounds you are hearing.
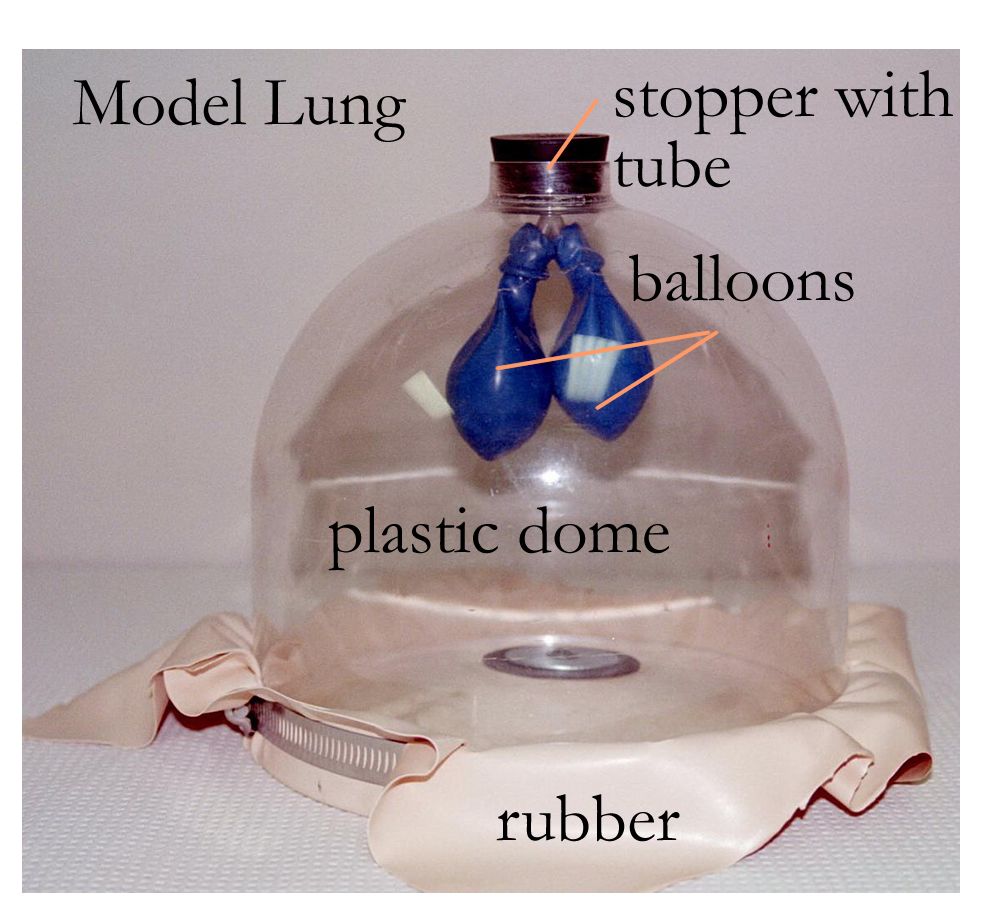
IV. Model lung : construct a lung using a paper lunch bag, rubber bags and various materials for the airways. Note how easy or difficult it is to inflate the lunch bag with each model you construct.
1. Model # 1: Use an empty paper towel roll. Place the lunch bag over one end covering about an inch of the roll and secure it with a rubber band. Take a normal breath and see if you can inflate the bag. Repeat taking a deep breath and see if you can inflate the bag.
2. Model #2: Use an empty toilet roll. Place a second unused lunch bag over one end covering about an inch of the roll and secure it with a rubber band. Take a normal breath and see if you can inflate the bag. Repeat taking a deep breath and see if you can inflate the bag.
3. Model #3: Use a clean drinking straw. Place a third unused lunch bag over one end covering about an inch of the straw and secure it with a rubber band. Take a normal breath and see if you can inflate the bag. Repeat taking a deep breath and see if you can inflate the bag.
4. Model #4: Use notebook paper to make a tube. Roll it into a tube starting at one of the short ends to create a one inch diameter for the final tube. Use scotch tape to secure the rolled ends. Place a fourth unused lunch bag over one end of the paper tube, covering about an inch on that end. Secure with tape, forming a tight seal. Take a normal breath and see if you can inflate the bag. Repeat taking a deep breath and see if you can inflate the bag.
5. Model #5: Take Model #4 and create a small hole (1/2 inch) in the bag. Repeat the experiment breathing into the lung model with a normal and deep breath.
Which lung model was easier to inflate ? Which lung model required a deep breath to inflate ? What does the length of the tube have to do with ease of inflation ? What does width of the tube have to do with ease of inflation? How might these models mimick certain respiratory diseases ?
V. Blood Gas Values were given earlier for PCO2 (~ 40mmHg) and PO2 (~90 mmHg)
In restrictive lung diseases, both the PCO2 and PO2 decrease, while in obstructive lung diseases the PCO2 increases and the PO2 decreases. Explain why this might happen.
Concept
Map: Make a concept map of the respiratory system (histo and gross) anatomy
and physiological function. Include instruments used to measure the respiratory
volumes during pulmonary ventilation.
This concept map is part of the LAR lab
report
(if selected), so include
as a document insert or as an additional PDF scanned document.
Hyaline membrane disease Asthma
Pneumothorax Emphysema
Epistaxis (nose bleed) Sinusitis
Laryngitis Tonsillitis
Croup Adenoid Hyperplasia
Heimlich maneuver Atelectasis
Pulmonary edema Pneumonia
Pleurisy (Pleuritis) Pleural Effusion
Carbon Monoxide Nitrogen Narcosis
Bronchiectasis Bronchitis
Lung Cancer Pulmonary Fibrosis
Cystic Fibrosis Pulmonary Embolism
Respiratory Distress Syndrome Pulmonary Edema
Whooping Cough (pertussis) Pneumoconiosis
Chronic Obstructive Pulmonary Disease (COPD) Cor Pulmonale
Sudden Infant Death Syndrome (SIDS) Respiratory Mycoses
Legionnaire’s Disease Lung Abscess
Respiratory Therapist
http://www.nlm.nih.gov/medlineplus/healthtopics.html
http://www.lumen.luc.edu/lumen/meded/histo/frames/histo_frames.html
http://www.gen.umn.edu/faculty_staff/jensen/1135/webanatomy/
http://gened.emc.maricopa.edu/bio/bio181/BIOBK/BioBookTOC.html
http://www.kcmetro.cc.mo.us/maplewoods/Biology/Bio110/Labs.htm
http://calloso.med.mun.ca/%7Etscott/second.htm
http://www.track0.com/canteach/links/linkbodysystems.html
http://www.carr.lib.md.us/schs/science/anatomy/systems.html
http://www.innerbody.com/htm/body.html
http://www.lung.ca/copd/anatomy/index.html
http://edcenter.med.cornell.edu/CUMC_PathNotes/Respiratory/Respiratory.html
http://sln.fi.edu/biosci/systems/respiration.html
http://gened.emc.maricopa.edu/bio/bio181/BIOBK/BioBookRESPSYS.html
http://www.leeds.ac.uk/chb/lectures/anatomy7.html
http://www.stemnet.nf.ca/CITE/body.htm
http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm
http://www.stemnet.nf.ca/~dpower/resp/main.htm
http://www.lung.ca/lunghealth/
http://www.lungusa.org/learn/resp_sys.html
http://www.holistichealth.com/respiratory/respiratory.html
http://biology.clc.uc.edu/courses/bio105/respirat.htm
http://www.cyber-north.com/anatomy/respirat.htm
http://www.mfg.mtu.edu/cyberman/environment/air/anatomy.html
http://www.cayuga-cc.edu/about/facultypages/greer/biol204/resp3/resp3.html
http://webmd.lycos.com/content/dmk/dmk_article_1459232
http://personal.wofford.edu/~shifletgw/RespDis.HTM
http://www.umm.edu/respiratory/anatomy.htm
http://www.quia.com/fc/2750.html
http://www.medem.com/medlb/article_detaillb.cfm?article_ID=ZZZQZDECGJC&sub_cat=198
http://www.medem.com/MedLB/article_detaillb.cfm?article_ID=ZZZ8PPLCGJC&sub_cat=285
http://www.nlm.nih.gov/medlineplus/lungsandbreathing.html
1. Define respiration
2. Be able to identify and give the function for the
Nasal Cavity
Pharynx
Larynx
Trachea
Bronchi
Bronchioles
Alveoli
Lungs
3. Give the structure and function of the pleura
4. Name two central and peripheral controls for respiration
5. Name the four phases of respiration and define each.
6. What is partial pressure of a gas?
7. Name two respiratory volumes and a capacity and define each.
8. How are gases transported in the blood?
9. What is the respiratory membrane and how do gases move?
10. How does inspiration occur?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}